Chronic Kidney Disease
Patient with history of obesity, HTN, and DM type 2 presents with decreased renal function for > 3 months. Decreased urine output, continued unhealthy diet, and progression of diabetic retinopathy on yearly ophthalmologic exam. Denies recent illness, flank pain, pruritic rash. Denies family history of renal disease. HTN with decreased visual acuity on exam. No JVD, M/R/G, abdominal bruit, flank pain, suprapubic tenderness, LE edema, joint swelling/tenderness, rash on exam. Dorsalis pedis pulse 2+ bilaterally.
Labs
Obtain CBC, CMP, lipid panel, HbA1c, urinalysis, urine culture, morning spot urine albumin/creatinine ratio; GFR calculated using National Kidney Foundation (NKF) calculator <60 mL/min/1.73 m^2
Hgb indicates anemia: Obtain reticulocyte count, ferritin level, transferrin saturation, and vitamin B12/folate levels
No urine sediment or casts noted on microscopy
Imaging
Obtain renal ultrasound with Doppler to rule out structural disease, decreased perfusion
Consider nerve conduction study if pt develops paresthesias or s/sx consistent with restless leg syndrome
Blood pressure management per KDIGO for adults with and without DM
Hypertension and not pregnant: Start lisinopril 2.5 (GFR < 30) to 10 mg (GFR > 30) qd for renal protection and titrate to 40 mg daily with close monitoring of serum potassium and creatinine
Albumin-creatinine ratio
< 30 mg/24h: Treat to ≤ 140/90 mmHg
≥ 30 mg/24h: Treat to ≤ 130/80 mmHg with at least one ACE-I or ARB
Monitor for postural hypotension
Treatment per stage (KDIGO recommendations, see notes for shared decision making considerations)
All patient stage ≥ 3a (GFR < 60)
Obtain annual CBC (anemia) and baseline CMP, phosphorous, PTH
Serum bicarbonate < 22 mmol/L: Start oral bicarbonate supplementation
Elevated PTH: Obtain serum 25-hydroxyvitamin D and supplement to > 20 ng/mL
Administer pneumococcal 23 vaccination
Refer to nutrition to discuss caloric, protein, sodium, potassium, and phosphate intake
Stage 3b (GFR 30-44)
Obtain annual CMP, serum phosphate
Do not perform routine bone mineral density testing (risk for misleading results)
Maintain serum phosphate concentrations within normal range
Stage 4 (GFR 15-29)
Obtain CBC every 6 months
Immunize against hepatitis and confirm response with HBV Ab
Do not administer bisphosphonate therapy
Prepare for renal replacement therapy
Stage 5 (GFR < 15): Refer to nephrology for initiation of dialysis
Medication
GFR < 60: Avoid sodium-phosphate bowel preparations
Uremic pruritus: Chronic condition common in advanced CKD. Trial of capsaicin cream and/or mirtazapine.
Refer to nephrology for any of the following:
GFR <30 mL/min/1.73 m^2
Potassium levels persistently > 5.0 meq/L
Two of three early morning spot urine albumin/creatinine ratio > 300 mg/g and spot urine protein/creatinine ratio > 500 mg/g
Development of anemia of chronic disease
Imaging with contrast: Hydrate before/after study and reevaluate GFR within 48-96 hours
Notes
Diagnosis
Differential includes alternate etiologies that may be indicated by recent illness, urine sediment/casts on microscopy, etc.
Acute: AKI (Cr 1.5-1.9 x baseline or Cr increase > 0.3 mg/dL), UTI, nephrolithiasis
Chronic: Autoimmune disease, familial kidney disease
Acute or chronic: Medication use, intrinsic renal disease
CKD diagnostic criteria: Must meet one of the following for > 3 months
GFR < 60 ml/min/1.73 m^2
Any marker of kidney damage: Albuminuria ≥ 30 mg/24 hours, electrolyte/urine sediment/structural/histologic abnormality, history of renal transplant
Source: KDIGO Practice Guidelines
Determining Renal Function
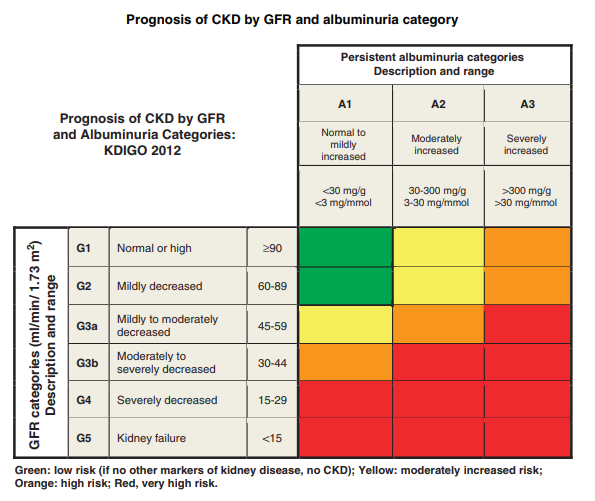
CKD categorized per GFR (see KDIGO chart, NKF calculator) and albuminuria
Creatinine
Creatinine concentrations affected by muscle mass/protein intake and may be less reliable in frail/aging populations
If concern for Cr accuracy, consider cystatin C for confirmation (e.g. GFR 45-59 with no marker of kidney damage)
If GFR per Cr and cystatin C < 60, diagnosis is confirmed
Albuminuria
Term “microalbuminuria” no longer recommended
Spot urine albumin/creatinine ratio (ACR)
Can be collected at any time
Confirm ACR ≥ 30 mg/g with early morning urine sample
Greater values indicate increased risk for progression to ESRD and death
Suspicion for false elevation due to multiple myeloma: Obtain urine kappa/lambda light chain assay (Bence-Jones protein)
Only used for medication adjustments
Calculation becomes increasingly important in elderly patients as GFR declines with age. For example, in two 70 kg male patients with Cr 1:
GFR in the 40 y/o = 44 mL/min
GFR in the 80 y/o = 26 mL/min
Dialysis Considerations
Patients with CKD have variable illness trajectories
Dialysis inconsistently modifies symptoms (i.e. patient dependent)
Mortality is significantly affected by patient characteristics
Average annual mortality for hemodialysis patients is 20%
Dialysis may not prolong survival in the frail/elderly or those with significant comorbidities
Calculators