Gastrointestinal
Gastrointestinal
Pt with h/o liver cirrhosis, portal hypertension, varices presents with acute onset hematemesis. Varices diagnosis previously established during q3 year screening endoscopy. Active hematemesis with bright red-blood, gynecomastia, hepatomegaly, caput medusa on exam.
Obtain CBC, CMP, PT, PTT, INR, FOBT
Surgery consult for urgent EGD; may require banding
Start octreotide 50mcg IV bolus followed by 25mcg/hour IV x2 days
Bactrim SS BID x 7 days
H/o previous variceal bleeds; consider TIPS procedure s/p stabilization
Discharge with prophylactic propranolol 40mg BID
Propranolol contraindicated; start isosorbide mononitrate 20mg BID
Yearly EGD due to established variceal diagnosis
Pt counseled about significantly elevated risk for re-bleed during 6 weeks following discharge
Pt advised that long-term therapy may involve liver transplant
Rate of variceal bleeding in patients with established diagnosis is 10-30% per year
For patient's with Bactrim allergy, use Norfloxacin
Pt with h/o NSAID use presents with dyspepsia. Denies unexplained weight loss, dysphagia/odynophagia, recurrent vomiting, family history of gastrointestinal cancer, overt gastrointestinal bleeding. No conjunctival pallor, abdominal mass on exam.
Obtain H. pylori fecal antigen testing
[Pt <55 y/o with no alarm symptoms; endoscopy not indicated]
Triple therapy x14 days: PPI 20mg BID, amoxicillin 1g BID, clarithromycin 500mg BID
Follow-up in 1 month and repeat fecal antigen testing if symptoms persist
Failed triple therapy; start PPI 20mg BID, metronidazole 500mg TID, tetracycline 500mg 4x daily, bismuth sbsalicylate 524mg 4x daily
Pt <55 y/o with h/o GERD, IBS, anxiety/depression presents with chronic, paroxysmal epigastric pain associated with early satiety. Symptoms started 6 months ago and have been persistent during past 3 months. Abdominal pain does not radiate to chest/back/RUQ and is not relieved by flatus. Pt cannot finish normal size meals multiple times per seek due to sensation of bloating/nausea. Denies excessive alcohol use and red flags including unintended weight loss, progressive dysphagia, persistent vomiting, dark tarry stools, BRBPR. No family h/o GI malignancy. Pain with palpation of epigastric region on exam.
Obtain CBC, BMP, H. pylori fecal antigen testing
Treatment
CrCl >50 mL/min: Start ranitidine 150 mg BID
Positive H. pylori fecal antigen test: Triple therapy with omeprazole 20 mg BID, amoxicillin 1 g BID, and clarithromycin 500 mg BID x 14 days
Refractory symptoms
Negative H. pylori fecal antigen testing: Consider starting metoclopramide 5 mg TID; pt counseled that medication should not be taken for greater than 12 weeks due to risk for tardive dyskinesia
H. pylori fecal antigen testing and s/p triple therapy: Consider quadruple therapy vs. referral for EGD (see PUD)
Pt advised to schedule follow-up appointment to address anxiety/depression
Affects 40 percent of adults yearly
Responsible for 70% of dyspepsia cases; differential also includes
Peptic ulcer disease (~20%)
Reflux esophagitis (~10%)
Esophageal/gastric CA (~2%)
Diagnosis
CBC screens for anemia that may occur due to GI bleed
Rome III criteria separates condition into disorders of epigastric pain and postprandial fullness
Intervention
Ranitidine
If not already documented, calculate creatinine clearance before starting BID
CrCl <50 mL/min: Start 150 mg qd
Metoclopramide (Reglan): Use with caution in older adults
Consider endoscopy and/or colonoscopy for patients older than 55 years and/or those with red flag symptoms
Non-pregnant patient with no h/o GI disease, endocrine disease, or radiation therapy presents with acute onset diarrhea. Describes increased stool frequency, volume, and water content x 2 days. Additional symptoms include thirst, lightheadedness, vomiting, and decreased urine output. Reports recent consumption of unpurified water/undercooked meat and antibiotic treatment while hospitalized in a developing nation. Sick contacts include child who attends daycare. Acute weight loss, dry mucous membranes, hyperactive bowel sounds, and mild/diffuse abdominal tenderness on exam.
Diarrhea lasting > 7 days with h/o immunosuppression, bloody stools, or fever: Obtain fecal lactoferrin (if positive, obtain stool cultures +/- analysis for stool ova/parasites)
Hospitalization with previous 3 days or antibiotic treatment within past 3 months: Test for C. difficile toxins A and B
Treatment
Oral rehydration therapy with 1/2 teaspoon salt and 6 teaspoons sugar mixed in 1 liter of water
BRAT (bananas, rice, applesauce, toast) diet until symptoms improve
Sensation of bloating/gas pain: Start simethicone 80 mg TID PRN
Non-bloody diarrhea: Start loperamide 2 mg q4h PRN, maximum 16 mg/day
Fever and/or bloody diarrhea: Trial of Pepto-Bismol
Patient advised that lactobacillus 1 to 4 packets qd may shorten illness duration
Antibiotics
C. difficile: Vancomycin 125 mg PO q6h x 10 days
Elderly, immunocompromised, or severely ill: Empiric ciprofloxacin 500 mg BID x 3 days
Recent travel: Azithromycin 500 mg qd x 5 days (Asia) vs. ciprofloxacin 500 mg BID (other continents)
Giardia: Metronidazole 500 mg TID x7 days
Pt counseled about importance of hand washing to prevent infection of others
Schedule follow-up appointment is symptoms last > 14 days
Etiology
Viral gastroenteritis is the most common etiology
C. difficile should be suspected s/p recent hospitalization
Advanced organizer for bacterial causes of bloody (inflammatory) diarrhea: You’re Constantly SShitting EErythrocytes
Yersinia
Campylobacter
Salmonella (non-Typhi), Shigella
Enteroinvasive E. coli, Entamoeba histolytica
Consider giardia in pt with recent consumption of unpurified water, e.g. while camping
Additional risk factors
Recent treatment with antibiotics
Exposure to high-risk individuals, e.g. children in daycare
Travel in underdeveloped nations
Special populations
In children, presence of two or more of the following indicates > 5% fluid deficit and need for oral rehydration therapy: Capillary refill > 2 seconds, absence of tears, dry mucous membranes, generally ill appearance
Pregnant patients are at increased risk for listeriosis
Immunocompromised patients are at greater risk overall
GI/endocrine disease and treatment with radiation therapy may cause gastroenteritis, but are beyond the scope of this vignette
Lactoferrin: Marker for fecal leukocytes (sensitivity 90%, specificity 70%)
Female pt with h/o functional abdominal pain presents with acute on chronic abdominal pain x6 months. Cramping pain has occurred ≥3 days per month during the past 2-3 months (see notes) and is associated with change in frequency/consistency of stools. Pain improves with defecation, but pt often experiences sensation of incomplete evacuation. Mucous sometimes present in stool, but no hard/bloody/tarry stools. Denies fever, unintentional weight loss, dysphagia/dysphagia, vomiting, back pain, dysuria. No family h/o Celiac disease, IBD. Afebrile and appears anxious on exam.
Consider CBC, TSH, CRP, ESR
Rule out Celiac disease: Consider anti-tissue transglutaminase IgA
Rule out GI bleed/alternative diarrhea etiologies: Consider FOBT and/or fecal ova/parasite testing
Consider abdominal x-ray
Pain persisting for >1 year: Consider referral for EGD
Recommend exercise and CBT
Diarrhea-predominant symptoms
Hydrolyzed guar gum 5g qd
Peppermint oil capsules TID
Probiotics: Recommended Kefir PO
Refractory symptoms
Consider loperamide 0.25-0.5 mg/kg/day in 2 divided doses
Consider rifaximin 600mg
Constipation predominant symptoms: See pediatric functional constipation
Counseling for parents of pediatric patients
Parents advised to validate symptoms but avoid reinforcing symptoms with secondary gain, e.g. missing school
Parents counseled that symptoms generally resolve over the course of several months
Diarrhea and/or constipation predominant symptoms
Antidepressant: Fluoxetine 20 mg qd; increased to 40 mg qd for refractory symptoms
Antispasmotic: Dicyclomine (Bentyl) 20 mg 4 times daily x7 days; after 1 week, increase to 40 mg 4 times daily if necessary
Constipation predominant symptoms
Neomycin 4g qd
Lubiprostone (Amitiza): Start 8 mcg BID and increase to 24 mcg BID for severe, refractory symptoms
Peak onset occurs between 20 and 40 years old
1.5 times more common in females
Diagnosis
Based on Rome Criteria that include
Recurrent abdominal pain + two or more symptoms at least 1 day per week during the past 3 months
Additional symptoms include pain with defecation, change in stool frequency/form, etc.
Pediatric patients: Only 2 months of symptoms required vs. 3 months in adults
Describe stools using the Bristol Stool Scale
Most labs are not useful in diagnosis and should only be considered if history suggests an alternate etiology
30 y/o white F presents with history of smoking presents with abdominal pain, diarrhea and intermittent bright red blood per rectum for > 3 months. Abdominal pain is not exacerbated by meals and diarrhea sometimes occurs at night. Reports fever, unintentional weight loss, fatigue, abdominal pain, and arthralgias. Family history of first degree relative with inflammatory bowel disease. Medications include oral contraceptives and daily NSAIDs use. Weight loss > 5% over 3 months, scleral erythema, aphthous stomatitis, perirectal abscess/ulcer/fistula, intravaginal fistula, and erythema nodosum on exam.
Labs
Consider fecal calprotectin to rule out disease
CBC shows anemia
Obtain CMP, ESR, CRP, urine pregnancy test
Obtain ferritin, TIBC, folate level, and 25-hydroxyvitamin D level
Obtain stool studies including clostridium toxin A and B, ova & parasites, and stool culture
Obtain yearly Pap smear with HPV co-testing due increased cervical cancer risk
Imaging/Procedures
Initial workup
Toxic presentation: obtain CT abdomen and pelvis
Non-toxic presentation: Refer for colonoscopy with biopsy
Obtain colonoscopy every 1 to 3 years after diagnosis
Treatment
Crohn flare: Start prednisone 40 mg daily and taper daily dose by 10 mg/weeks until 20 mg qd and then taper by 5 mg/week until finished
Immunomodulators and/or biologics
Initiate per GI instruction
Administer PCV13 and PPSV23 if started
Start iron, vitamin D, and B12 supplementations
Administer HPV vaccine
Referrals
Refer to GI
Perianal involvement: Refer to colorectal surgery
Counseling
Patient advised that smoking cessations reduces associated complications
Patient counseled that she is at higher risk for nutritional deficiencies, osteoporosis, anemia, and thromboembolic events (e.g. DVT), and malignancy
Smoking, OCPs, and regular NSAID use increase risk for conditions
Patients diagnosed at age < 30 years often suffer greater complications
Increased risk for cervical, biliary tract, colorectal, and skin malignancies
Physical exam
Anterior uveitis and episcleritis (scleral erythema) may be present
Lesions may occur at any point along the GI tract
Fistulas from GI tract to vagina may form
Young adult with h/o recent abdominal infection presents with chronic abdominal pain. Pain associated with bloody diarrhea. ROS positive for blurred vision, arthritis. Reports diet rich in meats/fats and family h/o UC. Uveitis, aphthous stoma on exam.
Labs
Obtain CBC, ESR, CRP, FOBT, bacterial stool culture
Recent antibiotic use: Obtain C. difficile toxin PCR
Recent consumption of under-cooked beef: Obtain stool cx for E. coli O157:H7
Endoscopy/colonoscopy reveals contiguous inflammation limited to colonic mucosa; biopsy consistent with UC
Treatment: Refer to GI
Mesalamine
Disease limited to rectum: Start mesalamine 1g rectal suppository qhs
Extensive disease: Start mesalamine (Asacol HD) 1.6 g TID x4 weeks; continue 800 mg TID for maintenance of remission
Symptoms refractory to 5-ASA: Start budesonide (Uceris) 9 mg qd x8 weeks; consider adding probiotic E. coli 1917
Symptoms refractory to budesonide: Consider infliximab (Remicade) 5 mg/kg IV at weeks 0, 2, and 6; continue q8 weeks thereafter
Consider azathioprine 2 mg/kg/day for maintenance of remission
Counseling
Pt encouraged to call if experiencing fever, severe abdominal pain, 7 or more stools daily, and/or GI bleeding
Pt advised that cases of severe UC (>7 stools/day and elevated ESR) will require hospital admission for treatment with IV corticosteroids and/or surgical intervention
Pt counseled that she is at greater risk for cervical CA and osteoporosis
Pt counseled that UC increases risk for colon CA and that regular colonoscopies will be started within 10 years of diagnosis
Risk factors for UC include family history, living at higher latitudes in Western nations, diets high in meat/fat, and recent abdominal infection
UC-associated complications include uveitis (4%), aphthous stomatitis (4%), and arthritis (21%)
Normal ESR and CRP do not r/o UC
Medications
Mesalamine suppositories are more effective than oral formulations
Probiotic E. coli 1917 was shown to be as effective as mesalamine for achieving symptom remission
Azathioprine is a mercaptopurine derivative that acts to halt DNA replication
Pt with family h/o Celiac disease presents with acute, recurrent abdominal pain. Reports weight-loss, fatigue, N/V, recurrent mouth ulcers, abdominal bloating, diarrhea. Food diary shows symptom correlation with gluten-containing foods. Herpetiform rash on exam.

Dermatitis herpetiformis. By BallenaBlanca - Own work.
Initial diagnosis: Pt advised to keep a food diary/symptom log
Labs
Obtain CBC to r/o anemia
Anti-tissue transglutaminase IgA >10x ULN
Total IgA level WNL
Consider HLA DQ2, HLA DQ8, endomysial antibody testing
Elevated Anti-tissue transglutaminase IgA: Refer for endoscopy with duodenal biopsy
Counseling
Pt educated about elimination of dietary gluten including wheat, rye, and barley products
Recommend Celiac Disease Foundation’s guide to eating gluten free
Total IgA must be obtained to rule out IgA deficiency
Intestinal symptoms are significantly more common extraintestinal manifestations, e.g. dermatitis herpetiformis, anemia
8 y/o pt presents with acute onset abdominal pain. Pain started 24 hours ago in periumbilical region with radiation to RLQ. Pain now localized in RLQ and worse with coughing, movement. Reports anorexia, N/V. Fever, decreased bowel sounds, abdominal rigidity/guarding, RLQ pain with rebound tenderness on exam; positive psoas, obturator, and Rovsing signs.
Labs
CBC shows leukocytosis (WBC >10,000) with left shift (ANC >7,500)
Obtain CMP, CRP
Consider obtaining APPY1 panel, U/A, and/or beta-hCG
Imaging
Obtain abdominal ultrasound
Equivocal abdominal ultrasound: Consider clinical re-evaluation in 12 hours vs. abdominal CT with IV contrast pending calculated appendicitis risk (see below)
Calculate risk for appendicitis:
Children: Pediatric Appendicitis Score
Appendicitis suspected
Consult surgery
Morphine 0.1 mg/kg for pain control
Monitor for wound infection/post-surgical complications s/p procedure
Pt counseled that even with appropriate care, perforation occurs in ~20% of patients
Special populations
Appendicitis is less common in patients younger than 5 and may present differently
Appendix location changes during pregnancy and may alter exam findings
Exam maneuvers
Psoas sign: Pain elicited when pt lies on left side and examiner straightens and extends extends the R leg
Obturator sign: Pain with passive internal rotation of L thigh
Rovsing sign: RLQ pain with palpation of LLQ
Labs/Imaging
A normal WBC does not rule out appendicitis
Absolute neutrophil count (ANC) = [WBC * (% segmented neutrophils + % segmented bands)] * 10
APPY1 panel
Includes WBC, CRP, and myeloid reactive protein
Has prognostic value when combined with U/S, but may not be readily available some institutions
Choosing wisely: Avoid CT as first line imaging modality in pediatric patients
Treatment
New evidence suggests that uncomplicated cases can be treated with antibiotics; however, 40% of patients still require surgery within 1 year of treatment
Morphine does not increase perforation risk, but may only provide pain relief equivalent to placebo
Prompt surgical consult reduces perforation risk
40 y/o F with h/o low-fiber intake and diverticulosis presents in summer with acute onset abdominal pain. Reports fever, anorexia, nausea, LLQ abdominal pain (LR 3.3), dysuria. Denies vomiting (LR 1.4), regular physical activity. Medications include NSAIDs, steroids, and chronic PO analgesics. Obese with fever (LR 1.4), abdominal distention, and LLQ pain (LR 10.4) on exam. Hypoactive bowel sounds, abdominal rigidity, and rebound tenderness concerning for peritonitis.
Labs
Obtain BMP, U/A
CBC shows leukocytosis
C-reactive protein >50 mg/L
Imaging
Abdominal/pelvic CT with contrast shows inflamed diverticulum, arrowhead sign, fascial thickening, and free air
Abscess present: Consult for CT-guided percutaneous drainage; send aspirate for culture
Bowel obstruction, abscess, and/or perforation: Consult surgery and calculate mortality risk using Mannheim Peritonitis Index
Complicated disease: F/u 4-6 weeks s/p symptom resolution for colonoscopy
Treatment
Unable to tolerate PO, concern for complicated diverticulitis, and/or s/sx peritonitis: Admit inpatient
NS at 125 cc/hr while NPO
Start metronidazole 500 mg IV q8 hours; transition to PO at discharge
Start ceftriaxone 2g IV qd; transition to ciprofloxacin 750 mg BID at discharge
Counseling
Pt advised that 30% of patients require abdominal surgery while admitted
Pt counseled that dietary fiber, exercise, weight loss, and smoking cessation can help prevent future episodes
Pt counseled that avoiding nuts, corn, and popcorn will not reduce risk of future episodes
Epidemiology
Diverticulitis admissions are more common during summer months
Women at 2x greater risk for complications
Chronic NSAIDs, corticosteroid, and/or opioid analgesics increase perforation risk
Diagnosis
Localized LLQ pain is the most predictive physical exam finding (LR 10.4)
Arrowhead sign: Triangular colonic wall thickening pointing to diverticulitis
Severity
Complicated diverticulitis
Associated with one of the following diagnoses: Obstruction, phlegmon, abscess, fistula, perforation
Indication for hospitalization and IV antibiotics
Refer to a local antibiogram due to increasing E. coli resistance against fluoroquinolones and some 3rd generation cephalosporins
Uncomplicated diverticulitis:
Does not meet qualifications for complicated diverticulitis (>90% of cases)
Can be managed outpatient with rest and fluids
Antibiotics do not improve outcomes
Pt with h/o abdominal hernia, irritable bowel disease, intra-abdominal malignancy, and abdominal surgery presents with acute onset, generalized abdominal pain. Reports N/V. No flatus, bowel movement since abdominal pain began. Fever, abdominal distention, hypoactive high-pitched bowel sounds, tympany with abdominal percussion on exam.
CBC shows leukocytosis
CMP shows hypokalemic, hypochloremic metabolic alkalosis
Obtain serum lactate
Abdominal CT with IV contrast shows dilated small bowel loops proximal to obstruction with air-fluid levels >2.5 cm long and located at different heights within the same bowel loop (step-ladder distribution)
Uncomplicated bowel obstruction: Initiate bowel rest, abdominal exams q8 hours
Complicated bowel obstruction with evidence of vascular compromise, perforation, and/or closed loop obstruction: Obtain immediate surgical consult
Start normal saline at 125 cc/hr
Fever and leukocytosis: Start metronidazole 500 mg IV q8 hours, ciprofloxacin 400 mg IV BID
Significant N/V and/or abdominal distention: Initiate decompression with NG tube
Presence of intra-abdominal malignancy: Consult hematology/oncology
Diet: NPO
Notes
Greatest risk factor is mechanical occlusion
Up to 75% of cases are due to surgical adhesions
Hernia, luminal masses due to IBD, and malignant may serve as nidus for obstruction
Strangulated hernia can lead to vascular compromise
Closed loop obstruction etiologies include intestinal volvulus
Pt >60 y/o with h/o CAD, AFib, PAD, ESRD, hypercoagulability, and smoking presents with paroxysmal abdominal pain out of proportion to physical exam. Pain worse after eating and/or snorting cocaine. Receives outpatient dialysis three times weekly and is s/p recent vascular surgery including CABG. Fever, tachycardia, tachypnea, leukocytosis, JVD, bilateral lung crackles, irregularly irregular heart rhythm, diffuse abdominal tenderness to palpation, and LE pitting edema on exam.
Obtain CBC, CMP, lactic acid
FOBT negative
Obtain magnetic resonance angiography
Treatment
Consider GI decompression
Start normal saline at 125 cc/hr
Start IV morphine 3 mg q4h PRN pain control; titrate as necessary
Etiology specific
Arterial occlusion identified: Consult surgery for potential laparotomy with embolectomy
Non-occlusive: Eliminate vasoconstricting medications and consider starting nitroglycerin 0.4 mg sublingual for acute pain
Start anticoagulation with apixaban (Eliquis) 5mg BID
Risk factors
Conditions that reduce peripheral circulation, e.g. sepsis, HF
CABG → transient hypoperfusion during procedure and increased risk for thromboemboli
Cocaine → vasoconstriction
Dialysis increases risk for non-occlusive mesenteric ischemia
Intestinal bleeding is uncommon early in the disease process
Start vasodilating agents if needed, but avoid vasoconstricting agents that may reduce blood supply
Pt with h/o constipation/straining presents with rectal bleeding. Hemorrhoid visible on exam.
Refer for colonoscopy due to [FOBT+, iron deficiency anemia on CBC]
Age>50 and no colonoscopy within the past 10 years: refer for colonoscopy
Age>40 and no colonoscopy within the past 10 years with one 1st degree relative diagnosed with colorectal CA prior to age 60: refer for colonoscopy
Age>40 and no colonoscopy within the past 5 years with more than one 1st degree relative diagnosed with colorectal CA prior to age 60: refer for colonoscopy
Topical nifedipine/lidocaine for pain relief
Stool softener, fiber supplementation
Discussed importance of adequate fluid intake
Refer to surgery: Concern for thrombosis due to acute onset of severe pain
Pt with h/o abdominal surgery presents with paroxysmal epigastric/umbilical discomfort. Pain occurs at site of protrusion extending from the abdominal wall; worse with coughing/straining. Denies fever, chills, anorexia, unintended, weight loss, change in bowel habits, diarrhea, dark/tarry stools, BRBPR. Abdominal wall protrusion reducible and resolves while pt is supine.
CBC WNL
Obtain ultrasound if unsure of diagnosis
Non-incarcerated: Refer to general surgery for elective repair
Pt counseled that smoking cessation, weight loss to achieve BMI <50 kg/m^2, and glucose control to achieve HbA1c <8% may be required prior to elective surgery
Pt advised to contact provider if experiencing acutely increased abdominal pain associated with constipation and/or a non-reducible protrusion
Hernias can cause pain even without palpable protrusion in exam
Location of common hernia types
Associated with abdominal pain: Ventral midline
Sports hernias caused by twisting motion: Groin
A CBC may be obtained if there is concern for a rectus sheath hematoma (rare)
Health care professional with h/o HIV, IV drug use presents with acute onset jaundice. Reports recent needlestick at work and episode of sexual assault. ROS positive for fatigue, poor appetite, N/V, abdominal pain, and dark urine. Denies h/o hepatitis B vaccination. Low-grade fever, jaundice, RUQ tenderness, hepatosplenomegaly on exam.
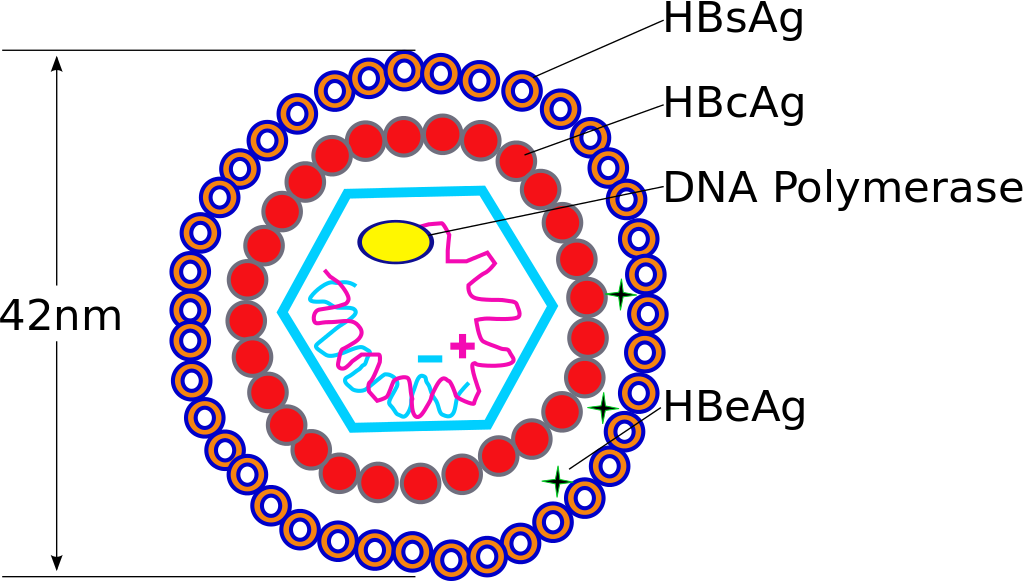
Hepatitis B virus. Source: Transferred by TimVickers from en.wikipedia, Public Domain
Labs
Positive HBsAg, anti-HBc, IgM anti-HBc
Negative anti-HBs
Obtain CBC, CMP, PT/INR
Obtain HBeAg, anti-HBe
Obtain HAV Ab, HCV Ab, hepatitis D Ab, HIV (ELISA Ag/Ab)
Imaging: Obtain RUQ U/S
Treatment: Refer to GI
Healthcare worker with needlestick exposure to HBV positive blood: Administer hepatitis B immunoglobulin and start hepatitis B vaccine series if not vaccinated
Newly diagnosed disease in HBeAg negative pt: Retest HBeAg in 6 months to determine if seroconversion to HbeAg positive state has occurred (see below for treatment of chronic hepatitis B)
Negative HAV Ab: Administer hepatitis A vaccine now and again in 6 months
Administer hepatitis B vaccine to other household members and any sexual contacts
Counseling
Transmission
Pt informed that HBV can be spread via intercourse, exposure to blood of an infected individual, and sharing personal items such as a toothbrush or razor
Pt reassured that HBV is not spread by casual contact (e.g. sharing food, kissing) or breastfeeding
Pt advised to stop drinking alcohol
Pt counseled that monitoring will include regular liver enzyme and HBV DNA level testing
Male pt born in a developing nation with h/o immunosuppression and ESRD requiring dialysis presents for routine health maintenance exam. Reports chronic injection drug use, regular sexual intercourse with men. Previous lab work shows elevated AST, ALT. No documented h/o hepatitis B vaccination. Household contacts include hepatitis B positive individuals. Plan: Obtain HBsAg and anti-HBc.
HBsAg negative, anti-HBc negative: Obtain anti-HBs to determine need for vaccination
HBsAg negative, anti-HBc positive: Obtain anti-HBs to verify immunity status
HBsAg positive, anti-HBc positive: Acute vs. chronic infection
Obtain IgM anti-HBc and anti-HBs to determine acute vs. chronic infection
Refer to sections on evaluation and treatment of acute (above) and chronic (below) hepatitis B infection
Evaluate for
History of co-infection with HCV, HIV
Personal/family h/o liver disease
History of alcohol use
Signs/symptoms active cirrhosis
Labs
Obtain HbsAg, anti-HBc, IgM anti-HBc, anti-HBs
Obtain HBeAg, anti-HBe, HBV DNA, and HBV genotype
Obtain HAV IgG, HCV Ab, hepatitis D Ab, HIV (ELISA Ag/Ab)
Evaluate liver function: Obtain CBC with diff, CMP, PT/INR
Referrals and Monitoring
Refer to GI for further evaluation
Pt informed that further workup/treatment may include liver biopsy, anti-viral therapy, and/or liver transplant
Counseling: See acute hepatitis B infection (above)
Yearly monitoring for cirrhosis: Obtain alpha-fetoprotein levels and RUQ ultrasound with liver elastography
Refer pt to surveillance program for hepatocellular carcinoma
Treatment
Treatment for patients without cirrhosis
HBeAg positive six months after initial diagnosis
ALT <2x ULN: Continue to monitor
ALT >2x ULN: Start tenofovir 300 mg qd and obtain HBeAg, anti-HBe monthly; continue for 4 months s/p conversion to anti-HBe positive state
HbeAg negative, HBV DNA >2,000 IU, and ALT > 2x ULN: Start tenofovir 300 mg qd and consider continuing treatment indefinitely
Treatment for patients with cirrhosis and HBV DNA >2,000 IU: Start tenofovir 300 mg qd and continue indefinitely
All other patients: Continue to monitor and/or defer to GI recommendations
Acronyms: HAV, (hepatitis A virus), HBV (hepatitis B virus), HCV (hepatitis C virus), Ag (antigen), Ab (antibody)
Screening
In general, all patients born in Africa and mainland Asia should be screened; see the CDC Yellow Book for all nations with a >2% infection list that qualify for screening
Common risk factors: Dialysis, immunosuppression, increased exposure (e.g. men who have sex with men, IV drug users)
Standard screening tests: HBsAg and anti-HBc
Acute hepatitis B
Liver failure occurs in 1% of patients
Risk for progression chronic disease is greatest in infants (90%) and decreases with age; only 5% of adults progress to chronic disease
Chronic hepatitis B
Considered chronic when infection persists >6 months
Each year, 1 in 400 HBV carriers die due to liver complications
Ultimate goal of treatment is to prevent initiation/progression of cirrhosis
Patients without cirrhosis: Initiation primarily determined by seroconversion to anti-HBe and evidence of liver damage
In cirrhosis patients: Initiation determined by evidence of active disease
Pt with h/o alcoholism, chronic viral hepatitis, NAFLD, DM type 2, autoimmune disease presents to establish care. Reports recent anorexia, weight loss, weakness, fatigue, abdominal fullness, pruritus. Fever, confusion, gynecomastia, abdominal distention, caput medusa, flank dullness with percussion, splenomegaly, Dupuytren's contracture, jaundice, spider angiomata, palmar erythema, asterixis on exam.
Labs
Liver function
Obtain CBC, CMP, GGT, PT, PTT, INR
CMP shows AST and ALT 2x ULN (consistent with values 6 months prior), elevated bilirubin
Hepatitis B screening
Obtain hepatitis B surface antigen (HBsAg)
If HBsAg positive: Obtain HBsAg antibodies (anti-HBs) and hepatitis B core antigen (anti-HBc)
Hepatitis C screening: Obtain HCV antibody test; if positive, obtain HCV RNA test
Concern for hepatic encephalopathy: Obtain ammonia level
Imaging
Ultrasound
RUQ U/S shows liver nodularity, irregularity, increased echogenicity, atrophy
Abdominal U/S shows abdominal ascites
Consider Doppler U/S of portal and hepatic veins
Consider abdominal CT to establish baseline assessment of hepatic nodules
Consider EGD to assess for esophageal varices
Treatment
Hepatic encephalopathy (hypersomnia, asterixis): Start lactulose 20 mg TID and titrate to 4 bowel movements daily
Beta blockers
Esophageal varices on EGD: Start nadolol 40 mg daily
Stop beta-blockers for MAP < 82 mmHg
Ascites
Limit sodium intake to < 2,000 mg daily
Start Bumex 1 mg daily
Paracentesis with > 5L fluid removed: Administer 6g albumin for each liter of fluid removed
Spontaneous bacterial peritonitis: Admit to hospital
Obtain ascitic fluid culture and PMN count
Obtain blood, urine, sputum culture
Start IV cefotaxime 2g q 8 hours
Administer IV albumin 1.5 g/kg for BUN > 30 mg/dL, Cr > 1 mg/dL, and/or bilirubin > 4 mg/dL
Referral
Consider liver biopsy to definitively establish diagnosis
Refer to GI to establish care
Concern for esophageal varices: Refer for EGD
MELD score ≥ 15: Consider referral to transplant center
Counseling
Stop drinking alcohol
Three month mortality rate per MELD score
Risk for ascites, spontaneous bacterial peritonitis, portal HTN leading to variceal bleeding and/or hepatorenal syndrome, hepatic encephalopathy
DM type 2 is a risk factor for NAFLD
Labs
Liver enzymes 2x ULN for 6 months is strongly correlated with cirrhosis on biopsy
If liver enzymes are normal and cirrhosis is suspected, consider ANA, anti-smooth muscle antibody
Anti-smooth muscle antibody is correlated with autoimmune hepatitis
Ammonia levels
Should only be obtained in the setting of altered mental status
Are not sufficient for the diagnosis if hepatic encephalopathy
Protein-restricted diets do not improve encephalopathy
Pt with h/o liver cirrhosis, right HF, Budd-Chiari syndrome, portal vein thrombosis presents with abdominal fullness. Reports weight gain, shortness of breath, early satiety. Weight increased from baseline, decreased breath sounds, flank dullness, abdominal fullness, shifting abdominal dullness/fluid wave on exam.
Obtain CBC, CMP, GGT, PT, PTT, INR
Abdominal U/S shows large-volume ascites
Obtain Doppler U/S of hepatic/portal veins
Paracentesis
Perform diagnostic/therapeutic paracentesis
Send ascitic fluid for differential leukocyte count, total protein level, a serum-ascites albumin gradient, fluid cultures
SAAG >1.1/dL indicating high likelihood of portal hypertension
Paracentesis >5L; consider albumin 10g/L albumin infusion
Treatment
Start oral spironolactone 100mg qd and titrate to 400mg/day
Consider adding furosemide 40mg/day and titrating to 160mg/day for refractory ascites
Serum sodium <125 mEq/L; fluid restrict to 1.5L/day
Refractory ascites and
May require transplant: Consider TIPS procedure
Not a candidate for paracentesis, TIPS, transplant: Consider peritoneovenous shunt
Pt advised to abstain from alcohol, restrict sodium to 2g/day
85% of abdominal ascites is due to portal hypertension
SAAG = serum-ascites albumin gradient = serum albumin - ascitic fluid albumin
For SAAG <1.1/dL; evaluate for peritoneal carcinomatosis vs. pancreatic ascites
Pt with h/o cirrhosis, ascites presents with abdominal fullness, malaise. Reports fever, abdominal pain, confusion. Fever, hypotension, altered mental status, gynecomastia, abdominal tenderness, hepatomegaly on exam.
Obtain CBC, CMP, GGT, PT, PTT, INR
Abdominal U/S performed prior to antibiotic administration shows ascites
Ascitic fluid sent for differential leukocyte count, total protein level, a serum-ascites albumin gradient, fluid cultures
Ascitic fluid neutrophil count > 250/mL: Start empiric cefotaxime 2g q8h
Treatment after starting empiric antibiotics
Concern for hepatorenal syndrome: Continue to monitor
Administer albumin 1.5g/kg within 6 hours of diagnosis and 1g/kg on day 3
Discharge with prophylactic Bactrim SS (400mg SMX + 80mg TMP) daily
Patient counseling
Abstain from alcohol
Long-term therapy may involve liver transplant
Bactrim or norfloxacin ppx recommended for patients who survive episode of SBP
Ascitic fluid neutrophil count > 250/mL is diagnostic of SBP and an indication for starting empiric antibiotics
Pt with h/o liver cirrhosis, portal hypertension presents with acute onset confusion. Family reports recent changes in memory, personality, concentration. Denies recent head trauma. Normal SPO2, impaired attention, decreased decreased response time bradykinesia, hyperreflexia, rigidity, myoclonus, asterixis on exam. MMSE score <24.
Obtain CBC, CMP, fingerstick, ammonia level, ABG, FOBT
Head CT shows no signs of intracranial bleed or acute pathology
Eliminate sedating medications
Start lactulose 30mL PO TID; titrate to 3 BMs/day, max dose 300mL/day
Confusion continues with lactulose 300mL/day; start neomycin 4g q6h; titrate to 12g q6h
Condition refractor to lactulose, neomycin; consider starting flumazenil
Pt advised to abstain from alcohol
Pt counseled that long-term therapy may involve liver transplant
Hepatic encephalopathy may be exacerbated by endogenous benzodiazepines
Flumazenil is a benzodiazepine receptor antagonist
Protein restricted diet does not improve symptoms
Pt with h/o alcohol abuse, liver cirrhosis, portal HTN presents with elevated serum creatinine. Reports recent oliguria. No history suggestive of nephrotoxic drug use, shock, infection, significant recurrent fluid loss. Gynecomastia, hepatomegaly, caput medusa on exam.
Obtain CBC, CMP, U/A, urine osmolality/sodium/protein; strict I&Os
Serum sodium <130, creatinine >1.5, creatinine clearance <40
U/A with <50 RBCs per HPF
Urine osmolality > plasma osmolality, urine sodium <10
No sustained improvement in renal function s/p discontinuation of diuretics, 1.5L isotonic saline bolus
Renal U/S shows no evidence of obstruction/parenchymal disease
Start midodrine 2.5mg IV and IV octreotide to achieve MAP increase of 15 mmHg or more
Consider dopamine 2 mcg/kg/min IV to induce renal vasodilation
Consider TIPS to reduce portal HTN
Pt advised to abstain from alcohol
Pt counseled that median survival is 3-6 months
Pt counseled that long-term therapy may involve liver transplant
Hepatorenal syndrome = functional renal failure in cirrhotic patients in the absence of intrinsic renal disease
Cirrhosis } portal hypotension } splanchnic vasodilation } decreased systemic circulation } renal vasoconstriction } decreased renal blood flow, GFR, urine output } azotemia } sodium/water retention
Midodrine is an alpha-1 agonist
MAP = mean arterial pressure = 1/3(systolic BP) + 2/3(diastolic BP)
TIPS = transjugular intrahepatic portosystemic shunt
40 y/o Native American F with h/o DM, HLD, grand multiparity presents with acute on chronic abdominal pain. H/o similar relapsing/remitting pain x2 years. Now experiencing sudden onset, steady RUQ pain that started s/p consuming a fatty meal, has lasted >6 hours, and was not relieved by a bowel movement. Endorses chills and initially tried NSAIDs for pain relief with positive effect. PMH includes rapid weight cycling. Medications include OCPs. Fever, obesity, and positive Murphy’s sign on exam.
CBC shows leukocytosis
Obtain CMP, amylase, lipase, and total bilirubin levels
Imaging
Initial U/S shows bile duct dilation
Equivocal U/S with suspicion for acute cholecystitis: Obtain CT with contrast to confirm diagnosis and rule out complications, e.g. perforation
CT contraindicated: Consider HIDA vs. magnetic resonance cholangiopancreatography (MRCP)
Ketorolac 10 mg q4 hours as needed for pain; maximum duration of therapy = 5 days
Surgery c/s recommends laparoscopic cholecystectomy (CCY) within 72 hours of admission
Choledocolithiasis with suspected cholangitis +/- gallstone pancreatitis:
Development of jaundice, hypotension, and altered mental status since admission
NS at 125 cc/hr while NPO
Start metronidazole 500 mg IV q8 hours and ceftriaxone 2g IV qd
Suspect pt will benefit from endoscopic retrograde cholangiopancreatography (ERCP); consult GI
Risk factors for gall stones include ethnicity, female gender, and medical history including pregnancies (fat, female, forty, fertile and from the Americas)
Murphy’s sign: Pain that causes pt to stop inhaling while examiner palpates RUQ
Biliary colic
Pain due to intermittent impaction of gallstones against gallbladder neck; usually resolves after 1-5 hours
Two-thirds of patients will progress to acute cholecystitis within 2 years
Elective cholecystectomy should be considered after more than one occurrence
Antibiotic ppx is not required in low risk patients undergoing elective CCY
Choledocolithiasis
Obstruction of bile duct by gallstone → bacterial infection → complications
Bacterial infection within bile duct (cholangitis) may present with
Charcot’s triad: Fever, abdominal pain, jaundice
Renaud’s pentad: Charcot’s triad + hypotension and altered mental status
Pt >55 y/o with h/o alcoholism, biliary colic presents with sudden onset epigastric abdominal pain radiating to the back. Reports N/V, recent abdominal trauma. Current medications include estrogen HRT, furosemide, valproic acid, azathioprine, sulfonamide/tetracycline abx. Scleral icterus, decreased bowel sound, abdominal tenderness/guarding on exam. Positive Cullen and Grey-Turner sign.
Clinical dx of pancreatitis due to abdominal pain + serum amylase and/or lipase* 3x ULN
Suspected alcoholic pancreatitis due to Lipase/amylase >4; obtain Mg2+ and phosphorus levels
Obtain initial CBC, CMP, LDH, lipid panel, U/A
CBC, CMP (BUN, glucose, CA), Mg2+ q12h for 48h s/p admission
Perform u/s exam; consider f/u with contrast CT
Treatment
Initial 20mL/kg LR bolus over 1hr, then 300mL/hr x48hr; maintain UOP > 0.5mL/kg
IV morphine 2mg q2h; titrate per sx
Initial bowel rest; consider NJ nutrition if prolonged bowel rest required
Transition to PO fluid, low fat diet when pain controlled
>30% necrosis on CT: Start abx ppx with imipenem/cilastatin
Procedures
Suspected gallstone; consult GI for ERCP and consider cholecystectomy
Infected necrosis/persistent fluid collections on CT; c/s for CT-guided aspiration vs. surgical debridement
Monitor for 48-72 hours; evaluation/prognosis per Atlanta, BALI, Ranson, or APACHE II criteria
Imipenem/cilastatin (Primaxin IV) decreases pancreatic necrosis infection, but does not decrease mortality
45 y/o pt with h/o alcoholism, documented genetic disorder, autoimmune disease including IBD, previous radiation therapy to abdomen presents with acute on chronic abdominal pain. New onset midepigastric postprandial pain that radiates to the back; some relief with sitting upright/leaning forward. Reports pale, foul-smelling, bulky, and difficult to flush stools. Weight loss, jaundice on exam.
Obtain CBC, CMP, amylase, lipase, lipid panel
Suspected autoimmune pancreatitis; obtain IgG4 serum antibody, ANA, rheumatoid factor, ESR
One time screen for vitamin D deficiency
Contrast CT showing pancreatic ductal calcifications; f/u mass lesions/weight loss/jaundice suspicious for malignancy with EUS + FNAB
Presence of complicated/symptomatic pseudocyst and biliary/pancreatic duct obstruction; perform ERCP
Pancreatic duct >7mm (large duct disease); consider pancreaticojejunostomy
Pancreatic head enlargement noted; consider pancreatoduodenectomy (Whipple)
Pain control with Tylenol, NSAID, narcotics
40,000u lipase for steatorrhea and malabsorption
Start PPI to reduce pancreatic enzyme deactivation by gastric acid
.dmrx for control of DM
Pt counseled about low fat diet, small meals for pain control
Pt encouraged to consider alcohol, tobacco cessation
Refer to GI
Note: Serum lipase, amylase are not specific for chronic pancreatitis
Mild
No organ failure, no local complications (fluid collection/necrosis), no systemic complications
Typically resolves in first week
Moderate if one of the following:
Transient organ failure (≤ 48 hours)
Local complications
Exacerbation of co-morbid disease
Severe: Persistent organ failure
1 point for each; obtain labs within 48h of admission
Blood urea nitrogen level ≥ 25 mg per dL (8.9 mmol per L)
Age ≥ 65 years
Lactate dehydrogenase level ≥ 300 U per L (5.0 μkat per L)
Interleukin-6 level ≥ 300 pg per mL
Mortality rates
+3 (>25%)
+4 (>50%)
At admission (1 point for each):
Age >55
Blood glucose >200
WBC >16,000
AST >250
LDH >350
Within 48 hours (1 point for each):
Serum Ca <8
Hematocrit drop >10%
PaO2 <60 mmHg
BUN increase >5
Base deficit > 4
Fluid sequestration >6L
Mortality prognosis
0-2 (2%)
3-4 (15%)
5-6 (40%)
7-8 (100%)

