
Pediatrics
Acute Otitis Media
Pt with personal and family h/o otitis media presents with acute onset ear pain. Parents report fever, irritability, poor feeding, and pulling/tugging/rubbing of the ear. Attends daycare; parents smoke at home. Bulging, erythematous/cloudy tympanic membrane with air-fluid level on exam.

Acute otitis media. By B. Welleschik - Own work, CC BY-SA 3.0
Amoxicillin 80 mg/kg/day divided every 12 hours x
10 days in children < 2 y/o
7 days children > 2 y/o
Refer for tympanostomy tube placement for either of the following:
3 or more episodes in the past 6 months
4 or more episodes in the past year
Parents advised that
80% of cases resolve within 3 days without antibiotics
Antibiotics increase risk of vomiting, diarrhea, rash
Note: No treatment and follow-up in 3 months is recommended for otitis media with effusion
Upper Airway Cough Syndrome (UACS)
A.K.A. Post-Nasal Drip
Pt >6 y/o with atopy presents with cough x4 weeks. Parents report rhinorrhea, nasal stuffiness, sneezing, itching. No wheezing, suspicion of foreign body aspiration. Afebrile with post-nasal drainage and cobblestoning of posterior pharynx on exam.
Pt > 2 y/o: Start intranasal fluticasone (Veramyst) 27.5 mcg/spray, one spray per nostril daily
Loratadine
Pt 2-6 y/o: Start loratadine 5mg qd
Pt > 6 y/o: Start loratadine 10 mg qd
Parents advised to make f/u appointment if no clinical improvement within 2 months
Notes
Chronic cough in children defined as > 4 weeks
UACS is estimated to be the 3rd most common cause of cough in children younger than 6 years
Asthma = 36%
Protracted bacterial bronchitis = 12%
Upper airway cough syndrome = 9%
Protracted Bacterial Bronchitis (PBB)
Pt < 6 y/o with h/o asthma presents with cough x 4 weeks. Parents describe wet/moist, productive nighttime cough that interferes with sleep, SOB, intermittent wheezing. Asthma symptoms well controlled before 4 weeks ago and parents deny exposure to any asthma triggers. Afebrile and well appearing with rattling lung sounds on exam.
CXR shows bilateral peribronchial accentuation with focal consolidated infiltrates; negative for foreign body aspiration
Start amoxicillin/clavulanate (Augmentin) x 2 weeks
Parents advised to schedule appointment if symptoms do not resolve s/p antibiotic course
Notes
Chronic cough in children defined as >4 weeks
PBB is estimated to be the 2nd most common cause of cough in children < 6 y/o (asthma = 36%, PBB = 12%, upper airway cough syndrome = 9%)
CXR showing bilateral peribronchial accentuation with focal infiltrates may indicate PBB or asthma
If untreated, PBB can result in bronchiectasis
See Chest 2017; 151:884 and Ann Thorac Med. 2018 Jan-Mar; 13(1): 7–13 for further information
Acute Bronchitis
Pt with no h/o asthma presents with acute onset cough. Symptom onset >10 days ago. No altered mental status, rhinorrhea, coughing paroxysms, post-tussive emesis. Afebrile with HR and RR WNL; no crackles on exam.
Not currently peak influenza season and presenting with intermediate influenza risk within 36h of symptom onset: Obtain influenza PCR
Unvaccinated pt with cough lasting >3 weeks and whooping sound s/p cough: Obtain B. pertussis PCR, serology
Low suspicion for PNA; do not obtain CXR
Treatment
Pt < 6 y/o: Parents cautioned against use of cough/cold preparation
Pt > 1 y/o: Parents encouraged to try dark honey
Adult Treatment
Pt encouraged to try dark honey, echinacea, pelargonium
Trial of dextromethorphan 20 mg q6 hours
Pt wheezing: Administer PRN albuterol inhaler and consider episodic high-dose episodic inhaled corticosteroids
Patient advised that symptoms can last up to 3 weeks; f/u encouraged to fill pocket prescription if symptoms do not resolve by this time
Notes
Etiology
90% of cases are due to viral infection
Common cold generally last < 10 days while acute bronchitis can last up to 3 weeks
Presence or absence of green sputum cannot be used to differentiate between viral and bacterial illness
Do not test for influenza during peak season or outside of flu season due to high pretest probability and low positive predictive value, respectively
Pertussis suspected with pt presents with coughing paroxysms, whooping sounds, post-tussive emesis, etc.
Treatment
Dextromethorphan is not effective for cough suppression in children
Using the term "chest cold" can reduce use of antibiotics
Bronchiolitis (RSV)
Patient < 2 y/o with h/o eczema and no h/o intubation presents in January with increased respiratory effort. Parents report 3 days of increasing cough and decreased oral intake. Sick contacts include siblings and other children at daycare. Initial SPO2 94%. Low grade fever, tachycardia, rhinorrhea, nasal flaring, dry mucous membranes, grunting, mild retractions, and wheezing/crackles on exam.

Obtain daily weights to assess hydration status
Do not obtain virus panel
CXR shows non-specific peribronchiolar cuffing, hyperinflation, and atelectasis
Treatment
Start supplemental (blow-by) oxygen to maintain SPO2 > 90%
Nasal suction bulb PRN; avoid over-suctioning and/or deep suction
Respiratory rate > 60 breath/min or unable to maintain sufficient PO intake: Administer fluids via IV and/or nasogastric tube
Weight > 2.7 kg (6 lbs): Acetaminophen q6h PRN fever
Age > 6 months, weight > 5.4 kg (12 lbs): Ibuprofen q6h PRN fever
Counseling
Parents counseled that symptoms typically peak at 2-3 days and last 7-10 days
Parents reassured that it is unlikely a child will be hospitalized during the full illness course
Parents educated about the importance of hand washing and avoidance of second hand smoke to reduce risk for future respiratory infection
Notes
Lower respiratory tract infection most commonly caused by respiratory syncytial virus (RSV)
Peak season: December through March
Prophylaxis
Palivizumab: RSV monoclonal antibody administered monthly during peak RSV season (maximum 5 doses)
Administer to infants
Born before 29 WGA
Born before 32 WGA with chronic lung disease of prematurity
With hemodynamically significant heart disease
Diagnosis and treatment
Respiratory virus panels (PCR) cost between $1,000 and $3,500 and do not change management
Routine CXR is not recommended
Continuous pulse oximetry is not required
Treatment such as albuterol, epinephrine, corticosteroids, and/or antibiotics are ineffective and should be avoided
Infants with respiratory rates > 60 breaths/min may demonstrate poor feeding and benefit from NG tube or IV hydration
Predictors of severity
Safe discharge predicted by age > 2 months, no h/o intubation, h/o eczema, initial SPO2 of 94%, and adequate oral intake
More concerning s/sx include tachycardia, evidence of dehydration (decreased weight, dry mucous membranes), and increased respiratory effort
Croup (Parainfluenza)
2 y/o pt born at 37 WGA and with no h/o intubation presents with acute onset cough and hoarseness. Parents report 2-3 days of low-grade fever and nasal congestion; symptoms typically worse at night. Parents deny possibility for recent foreign-body aspiration. Low-grade fever, tachypnea, nasal flaring, barking cough, inspiratory stridor, retractions, cyanosis, disorientation on exam. No drooling, wheezing, crackles noted.

Steeple sign. By Frank Gaillard - Own work.
Do not obtain respiratory virus panel at present; may reconsider if pt does not respond to initial treatment
CXR shows steeple sign
Treatment
Administer single-dose oral dexamethasone 0.6 mg/kg
Westley Croup Score 3 or greater: Administer 0.5 mL nebulized racemic epinephrine
Administer oxygen to maintain SPO2 >94%
Monitor for 2 hours; admit to hospital if no improvement after initial treatment
Parents counseled that symptoms typically peak at 48 hours and resolve after 1 week
Notes
Pathology: Virally-mediated swelling of larynx, trachea, and bronchi
Epidemiology
Most common between age 6 months and 3 years
Croup is responsible for 99% of acute onset stridor cases in children
75% of cases are due to parainfluenza virus
Risk factors for severe croup include prematurity, prior intubation, and age < 3 years
Differential
Absence of cough and presence of drooling should raise suspicion for epiglottis
Steeple sign is not sensitive or specific for croup
Nebulized epinephrine reduces length of hospital stay in severe cases
Pertussis (Whooping Cough)
Pt with no h/o DTaP or TDaP vaccination presents with cough and intermittent apneic episodes. Cough started > 2 weeks ago. Current symptoms include coughing paroxysms followed by whooping sound and emesis. Low grade fever on exam.
Cough duration
< 4 weeks: Obtain PCR and culture
> 4 weeks: Obtain serology
CXR shows no foreign body
Treatment
Cough duration < 3 weeks: Start azithromycin (see notes for dosing)
Cough duration < 6 weeks and pregnant pt with small infant who works in health care: Start azithromycin (see notes for dosing)
Start post-exposure prophylaxis for all close contacts
Pt and parents advised that pertussis is highly contagious
Notes
Due to risk of transmission, antibiotics are started within 6 weeks of cough for a pt who is pregnant, anyone working with infants, and healthcare workers
Close contact prophylaxis
Close contact definition: Regular, face-to-face exposure within 3 feet of the symptomatic patient.
Threshold for "regular" can change based on the individual’s risk for contracting the illness, e.g. would be lower for immunocompromised individuals.
Azithromycin dosing
Age 1-5 month: 10 mg/kg x 5 days
Children 6+ months: 10 mg/kg on day 1 then 5 mg/kg days 2-5
Adults: 500 mg on day 1 then 250 mg days 2-5
Functional Abdominal Pain
Pt with h/o physical/sexual abuse presents with acute on chronic abdominal pain. Denies fever, weight loss, vomiting, bloody stools. Reports anxiety, bullying at school. Appropriate progression along growth curve; no fever, CVA tenderness, HSM, abdominal mass, jaundice on exam.
Consider CBC, CRP, ESR, U/A, beta-hCG, total IgA, anti-tissue transglutaminase IgA, FOBT, and/or fecal ova/parasite testing
Consider abdominal x-ray to r/o fecal retention
Treatment
Start cognitive behavioral therapy
Start lactobacillus, lactol with pH-dependent peppermint oil
Child/adolescent > 40 kg: Consider trial of famotidine 20 mg BID
Consider trial of cyproheptadine
2-6 y/o: 2 mg q8h
7+ y/o: 4 mg q8h
If symptoms do not improve, consider referral to GI
Reassurance provided to family
Notes
Responsible for 90-95% of chronic abdominal pain in children
No evidence for fiber, amitriptyline, citalopram when treating pain
Abdominal Migraine
7 y/o pt with presents with acute on chronic abdominal pain. Pain can be diffuse or periumbilical with episodes lasting 2 to 72 hours and affecting normal activities. Reports associated unilateral H/A, photophobia, N/V, anorexia that worsen with stress, physical activity. Denies presence of blood in stool. Afebrile with pallor on exam.
Consider CBC, U/A, beta-hCG, FOBT
Initial treatment
Start Tylenol, ibuprofen for pain
Zofran for nausea
Persistent symptoms
Consider propranolol and cyproheptadine for prophylaxis
12+ y/o: Consider sumatriptan for acute pain
Counseling
Parents advised to validate symptoms but avoid reinforcing symptoms with secondary gain, e.g. missing school
Family counseled about appropriate sleep habits, hydration
Family informed that symptoms generally dissipate in early adolescence
Note: Responsible for 5-15% of chronic abdominal pain in children
Functional Constipation
4 y/o pt with no h/o irritable bowel disease presents with acute on chronic abdominal pain and constipation. Parents report voluntary stool retention, two or fewer BMs per week, hard/painful BMs, stools that obstruct toilet, and at least one episode of stool incontinence per week. Deny bloody stools, delayed meconium passage at birth. Large fecal mass in recutm, normal cremasteric/anal wink/patellar reflexes on exam.
Consider obtaining TSH, lead level, fecal occult blood testing
Consider abdominal x-ray
Treatment
Perform fecal disimpaction in office
Trial of dietary fiber, fruit juices (e.g. prune, pear)
< 4 months: 2 ounces diluted fruit juice
> 4 months: 4 ounces diluted fruit juice
Polyethylene glycol (Miralax)
< 18 months: 1 tsp qd
18 months to 3 years: 2 tsp qd
Weight-based: 0.8 g/kg/day in 8 ounces fluid; maximum 34 g qd
2+ y/o: Dulcolax 10 mg qd
Glycerin suppository daily
Counseling
Parents counseled about recognizing withholding behavior; regular toileting/incentive systems encouraged
Parents counseled to expect prolonged course with frequent relapses
Consider GI referral for persistent symptoms
Notes
Most common cause of abdominal pain in children
Diagnosed using Rome III criteria; vary based on developmental age
Treatment options for children
Osmotic/lubricant laxatives
Polyethylene glycol 3350 powder (MiraLax)
Lactulose (70 percent solution)
Sorbitol (70 percent solution)
Magnesium hydroxide (milk of magnesia)
Mineral oil
Stimulant laxatives
Senna
Bisacodyl (Ducolax)
Glycerin suppositories
Stool softener: Docusate
Enemas do not improve outcomes in children with severe constipation
Hirschsprung Disease
48 hour old infant with h/o trisomy 21, genitourinary anomalies, hearing impairment presents with delayed passage of meconium. Parents report bilious vomiting, decreased appetite. Fever, weight loss, abdominal distention, perforate anus, tight anal sphincter, empty rectum, squirt sign on exam.
Obtain CBC, CMP
Consider abdominal x-ray
Obtain anorectal manometry, rectal suction biopsy
Consider additional screening for congenital abnormalities of kidney/urinary tract (CAKUT)
Parents advised that definitive management will include surgery
Refer to pediatric surgeon
Notes
Most common cause of lower intestinal obstruction in neonates
Squirt sign is passage of stool with introduction of finger into rectum
Suction biopsy show intestinal aganglionosis extending 2-4 cm proximal to internal anal sphincter
Pediatric Infectious Diarrhea
Pt with no h/o inflammatory bowel disease and no recent infections/hospitalizations presents with acute onset diarrhea. Reports fever, N/V, abdominal pain. Recently returned from international vacation; family went swimming and consumed shellfish, raw milk, unpasteurized juice, undercooked meats/fish/eggs, and uncooked produce while abroad. Fever, dry mucous membranes, abdominal pain, joint pain, erythema nodosum on exam.
Labs
Obtain CBC, CMP
Obtain U/A to r/o HUS
Bloody stools with fever: Evaluate stool culture for Yersinia, Campylobacter, Salmonella enterica, Shigella, STEC
Pt > 2 y/o with exposure to abx within previous 12 weeks: Obtain C. difficile PCR
Diarrhea lasting > 14 days: Evaluate for parasitic infection
Pt with h/o AIDS: Obtain stool cultures for cryptosporidium, Cyclospora, Cystoisospora, microsporidia, Mycobacterium avium complex, and cytomegalovirus
Treatment
Maintain hydration: Recommend electrolyte maintenance solution (see notes for recipe) and/or apple juice mixed half-and-half with water
Pt younger than 3 months with recent international travel, fever ≥ 100.4°F, abdominal pain, suspected shigella infection: Start empiric azithromycin 10 mg/kg qd x 3 days (max/adult dose = 500 mg)
Parents advised that infectious diarrhea is generally self-limited
Notes
Etiology
Report any diarrhea potentially caused by food or water-borne illness to identify possible outbreaks
Post-infectious irritable bowel syndrome due to recent infection should be considered and ruled out
Bloody diarrhea
Bloody diarrhea mnemonic: You're Constantly SShitting Erythrocytes (Yersinia, Campylobacter, Salmonella/Shigella, E. coli)
STEC: Shiga toxin-producing E. Coli
Physical Exam
Assess patient's volume status on exam to identify possible dehydration, e.g. mucous membranes
Extraintestinal and/or post-infectious manifestations may include reactive arthritis, erythema nodosum, or glomerulonephritis
Treatment
Oral rehydration therapy recipe: Mix 6 teaspoons sugar + 1/2 teaspoon salt in 1 liter of water and boil; allow to cool before consumption
See JAMA article: Electrolyte maintenance solution vs. dilute apple juice
IDSA Criteria for Empiric Antibiotic Therapy
Pt < 3 m/o with suspected bacterial etiology
Suspected Shigella infection with abdominal pain and documented fever ≥ 100.4°F (38°C)
Recent international travel with temperature ≥ 100.4°F (38°C) and/or s/sx sepsis
Inguinal Hernia
1 y/o male pt with h/o intermittent, reducible inguinal mass presents with painful groin mass. Previously, mass increased in size with increased abdominal pressure, e.g. crying. Inguinal mass extending into scrotum on exam.
Consider ultrasound to verify presence of hernia
Treatment
Reducible inguinal mass; refer to surgery for evaluation
Non-reducible, tender groin mass with concern for incarceration; emergent surgical reduction indicated
Pt counseled about importance of follow-up with surgery
Notes
Reducible, non-incarcerated hernias: Non-emergent surgery referral
Reducible, incarcerated hernias: Repair should occur within 2-5 days
Intussusception
2 y/o pt with h/o Meckel's diverticulum presents with acute onset RLQ tenderness. Pain is colicky and parents report concomitant onset of vomiting, red stools. Palpable abdominal mass, currant-jelly stool in diaper on exam.
Obtain CBC, CMP
Ultrasound shows target sign at ileocecal junction
Perform pneumatic enema
Parent's advised that intussusception recurs in 10% of cases
Notes
Most common form of intestinal obstruction between 6 and 36 months of age
90% of classes occur at the ileocecal junction
Pneumatic (air) enema is diagnostic and therapeutic
Ovarian Torsion
Adolescent female with presents with severe, intermittent, unilateral, and non-radiating lower quadrant abdominal pain. Reports N/V. Denies fever, vaginal discharge, dyspareunia, menses complications. Unilateral abdominal pain with palpation, enlarged/tender adnexa on exam.
Obtain CBC
Ultrasound shows enlarged adnexa (ovary > 5cm) and decreased flow on doppler
Consult OBGYN for detorsion surgery
Note: In pediatric patients, torsion can occur in the absence of an ovarian mass
Duchenne Muscular Dystrophy (DMD)
6 y/o M with h/o delayed crawling/walking as compared to siblings presents with fatigue, falls. Pt had difficulty holding his head up as an infant. Parents first became concerned lower extremity muscle weakness when pt was 2-3 y/o. Calf pseudohypertrophy, lower extremity muscle weakness, scoliosis on exam.
Labs
Obtain serum thyroxine, TSH, vitamin D
Serum creatinine kinase between 3,000 and 50,000 U/L
Obtain genetic analysis to confirm diagnosis
Treatment
Vitamin D < 30 ng/mL; start vitamin D supplementation
Start prednisone 0.75 mg/kg/day to slow disease progression, improve outcomes
Regular, gentle exercise recommended to prevent disuse atrophy
Refer to pediatric neurology, pediatric cardiology
Decreased growth velocity: Refer to pediatric endocrinology
Parents advised that fatal complications are generally due to late pulmonary and cardiac involvement
Notes
Most common fatal disease affecting children
Head lag due to neck muscle weakness is a specific, early presentation
On average, two years elapse between initial parental concern and formal diagnosis
Rule out hypothyroidism as it can mimic DMD
If serum CK elevated but less than 3,000 U/L, repeat testing in 2-3 weeks
Patients are at increased risk of long-bone fracture due to decreased mobility, corticosteroid use
Scoliosis
![Scoliosis plain film. Source: Silverjonny [Public domain]](https://images.squarespace-cdn.com/content/v1/5acb26595ffd203815e5314f/1556184211075-Q6WVC5G9XT6MV06JRI5F/Scoliosis+Plain+Film.jpg)
Scoliosis plain film. Source: Silverjonny [Public domain]
Infantile idiopathic scoliosis: Generally resolves spontaneously
Juvenile idiopathic scoliosis: Greatest risk for progression
Adolescent idiopathic scoliosis
Most common presentation
Risk factors: Female sex, magnitude of curve
Obtain spine radiology to calculate Cobb angle
20-30 degrees: Refer to orthopedics due to risk for progression
30-40 degrees: Brace and observe
40+ degrees: Surgical correction

Scoliosis Cobb angle of 89 degreees. Source: Skoliose-Info-Forum.de
USPSTF Screening Recommendation: Grade D
Spondylolysis
Adolescent patient presents with back pain for > 3 weeks. Pain located at the level of L4-L5 and is worse with lumbar spine hyperextension. Patient actively involved in gymnastics, football, soccer, weightlifting, volleyball, dance. Hyperlordosis and limited flexion/extension on exam. Pain reproduced with single-leg hyperextension.
Obtain lumbar spine x-ray with AP/lateral/bilateral oblique views
Evaluate for stress fracture of pars interarticularis
Diagnosis uncertain s/p plain film: Consider lumbosacral SPECT scan
Treatment
Recommend relative rest from offending activity, NSAIDs for pain
Patient may return to full activity in 6 months
Consider referral to physical therapy after ruling out spondylolisthesis (see below)
Refer to orthopedics if symptoms persist
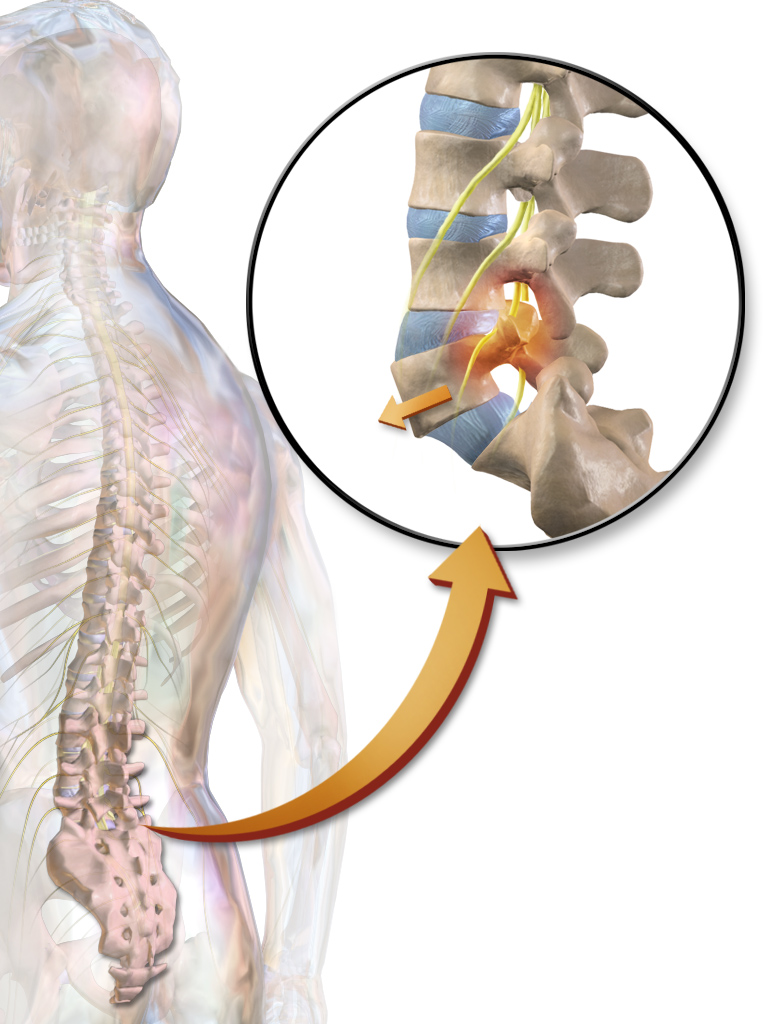
Example of spondylolisthesis: Anterior dislocation of L5 due to stress fracture in the pars interarticularis. By BruceBlaus - Own work.
Spondylolisthesis
12 y/o F gymnast presents with chronic and paroxysmal lumbar back pain. Chronic pain is a dull ache in the lumbar region. Paroxysmal pain is sharp, worse with extension (e.g. during back handspring), and radiates both laterally and into the buttocks. Paroxysmal pain sometimes accompanied by paresthesias in the back/buttocks and transient lower extremity weakness. Denies fever, chills, night pain, urinary retention, fecal incontinence. Kyphotic posture, hyperlordosis with anterior pelvic tilt, pain with deep L-spine palpation, hamstring/gluteal weakness, and positive Stark (single leg hyperextension) test on exam.
Imaging
Obtain plain anteroposterior (AP) and lateral radiograph of the lumbar spine and evaluate for fracture/vertebral displacement
Obtain MRI if plain films do not show pathology and
Pain persists after 2-3 weeks rest
Patient is an athlete and wishes to return to play
Imaging reveals spondylothisthesis: Refer to orthopedics for back brace x 6 weeks
Notes
Pathophysiology:
Stress fracture in pars interarticularis (spondylosis) leading to vertebrals displacement (spondylolisthesis)
Other sports related injuries may include serving/spiking ball in tennis/volleyball
Stark test
Patient stands on each leg and extends back
Considered positive if pain is elicited
Imaging
Consider repeating plain films if both x-ray and MRI are negative but pain persists for > 6 weeks
CT is not indicated
Little League Elbow (Medial Epicondyle Apophysitis)
11 y/o M with h/o arm/elbow injury presents with progressive medial elbow pain in while throwing. Patient pitches for multiple teams. Reports decreased pitching velocity, numbness/paresthesia in affected arm. Elbow swelling, decreased ROM of affected elbow, tenderness with palpation of medial elbow/distal arm/forearm on exam.
X-ray showing medial epicondyle hypertrophy/epiphyseal widening, loose cartilaginous bodies, osteochondral lesions
Ice, Tylenol, NSAIDs for swelling/pain
Complete rest from throwing for 4-6 weeks; restart with graduated throwing program.
May resume competitive throwing at 12 weeks; limit pitches to 200/week and 90/outing
Loose cartilaginous bodies/avulsion fracture on x-ray and/or failure of symptoms to improve after 12 weeks; refer to orthopedics
Osgood-Schlatter Disease (Tibial Tuberosity Apophysitis)
Adolescent pt with presents with anterior knee pain/swelling. Pt actively involved in soccer, basketball, gymnastics, volleyball. Tenderness/swelling of tibial tubercle on exam.
Plain x-ray shows fragmentation/irregular ossification at tibial tubercle
Treatment
Recommend rest from painful activities, icing, NSAIDs
Perform quadriceps stretching as part of strengthening program
May return to full activity in 6-8 weeks
Pt advised that residual bony deformity may occur
Sever's Disease (Calcaneal Apophysitis)
10 y/o with h/o participation in soccer, basketball, volleyball, track presents with activity-related pain in posterior heel. Parents report pt recently started a growth spurt. Tenderness with medial/lateral compression of posterior calcaneus on exam
Consider plain x-ray
Recommend activity modification, icing, gastrocnemius-soleus stretching, NSAIDs, and heel cushions
May return to pain-free activity in 3-6 weeks
Little League Shoulder
14 y/o M with presents with insidious-onset lateral shoulder pain. Pt plays baseball, tennis, and volleyball. Primarily throws breaking pitches, e.g. sliders, curveballs. Tenderness with palpation of proximal/lateral humerus on exam.
Bilateral AP shoulder x-ray in internal/external rotation show unilateral widening of the proximal humeral physis
Tylenol/NSAIDs for pain
Abstain from throwing/overhead sports for 3 months
Begin strengthening exercises when comfortable, interval throwing program when pain free
Parents advised that injury is generally self limited
Consider adequate rest periods, icing to prevent future episodes
Notes
Pathophysiology: Overuse injury resulting in epiphysiolysis of the proximal humerus
See OrthoBullets for more information
Hip Osteonecrosis (Legg-Calve-Perthes)
7 y/o Caucasian M with h/o low birth weight, perinatal HIV infection, sickle cell disease presents with insidious onset hip and knee pain. Parents report progressive, decreased hip ROM and intermittent antalgic gait; no fever. Decreased abduction and internal rotation of hip on exam.
Radiography showing femoral head lucency and subchondral sclerosis/collapse
MRI showing osteonecrosis of the femoral head
Refer to pediatric orthopedics
Notes
Risk factors
Age
May occur in patients age 2-12 years
Most common in children age 4-8 years
Poor prognosis in children older than 6 years
Sex: 5 times more common in boys
Race: More common in white as compared to black children
Pathophysiology: Avascular necrosis of the femoral head
Presentation
Pain can be referred to knee
Antalgic gait may be intermittent
Slipped Capital Femoral Epiphysis
13 y/o African American male with h/o obesity presents with deep hip pain while weight-bearing. Physical exam reveals antalgic gait with external foot rotation. Pain with log roll and straight leg raise against resistance. Pain with hip internal rotation relieved by external rotation.
Radiography shows posterior displacement of femur under epiphysis and through the epiphyseal (growth) plate
Refer to orthopedics
Patient and parents counseled that risk for avascular necrosis is 30% if not appropriately treated
Notes
Epidemiology
Most common in children ages 11-16 years
Risk factors: African American ethnicity, Male sex, obesity, physical activity
Pathophysiology: Femoral head displaced posteriorly through growth plate
Presentation
Pain generally anterior and within proximal third of thigh
Up to 33% of patients present with referred lower thigh or knee pain
Metatarsus Adductus
Newborn M with h/o prematurity presents with bilateral intoeing. Parents report twin sibling diagnosed with metatarsus adductus. Bilateral intoeing with kidney-shaped foot and deviated heel-bisector line on exam; forefoot abducts to neutral when heel placed in neutral position.
Treatment
Parents informed that imaging and treatment are generally not indicated
Severe metatarsus adductus in a child who is not walking; refer to pediatric orthopedics for adjustable shoes vs. serial casting x 6-8 weeks
Parents reassured that 85-90% of cases resolve by 1 year of age
Notes
More common in males, twins, and premature infants
Differential diagnosis
2% of cases are associated with developmental dysplasia of the hip
In metatarsus varus (rare), the forefoot does not abduct to neutral when heel is in neutral position
Severity determined by heel bisector line (normal = 2nd toe)
Mild = 3rd toe
Moderate = between 3rd/4th toes or on 4th toe
Severe = between 4th and 5th toes
Adjustable shoes are effective and less expensive than casting in pre-walking patients with motivated parents
Surgical correction is contraindicated due to high failure and complication rates
Internal Tibial Torsion
3 y/o pt with h/o frequent falls presents with bilateral intoeing. Forward facing patellae with feet pointing inward on exam.
No suspicion for rickets, Blount disease, or skeletal dysplasia; do not refer for imaging
Consider surgery if thigh-foot angle is greater than 15 degrees at age 8 years
Parents informed that braces and orthotics are ineffective
Parents reassured that most cases resolve by age 5 years and 90% resolve by age 8 years
Notes
Most common cause of intoeing overall
Most common between ages 2-4 years
Femoral Anteversion
5 y/o F with h/o sitting in W position, clumsy gait presents with bilateral intoeing. Parents report family h/o femoral anteversion. Increased internal hip rotation (60 to 90 degrees) with reduced external hip rotation (10 to 15 degrees), inward pointing feet/patellae, bilateral intoeing, and circumduction gait on exam.
Consider surgery at age 8 years for severe functional or cosmetic abnormality
Parents informed that radiography in not recommended and that braces/orthotics are ineffective
Parents reassured that 80% improve/resolve by 10 years of age
Notes
Most common cause of intoeing in school aged children
Diagnosed based on increased internal hip rotation and decreased external hip rotation
Fever in Infant 0 to 90 Days
Infant < 29 Days
Pt presents with sudden onset fever > 38.5 C. Parents report cough, increased WOB, diarrhea with blood/mucus in stool. Parents concerned about decreased oral intake, decreased production of wet/dirty diapers. Fever, tachypnea, grunting, nasal flaring, retractions, decreased responsiveness on exam.
Obtain CBC, BMP, blood culture, U/A with culture
Obtain CSF cell count/differential, glucose, and protein
Obtain CSF bacterial culture and enterovirus PCR
Obtain procalcitonin, CRP for risk stratification
Additional tests
Presenting during influenza season: Obtain influenza PCR
Respiratory distress: Obtain CXR
Diarrhea: Obtain stool culture
Treatment
Admit to hospital and start empiric coverage with cefotaxime, ampicillin
Positive influenza PCR and within 48h of symptom onset; consider oseltamivir 3 mg/kg/dose BID x 5 days vs. supportive care
Supportive care
Maintain adequate hydration
Titrate oxygen to maintain saturations > 92%
Notes
Empiric antibiotic doses vary depending on the child's age and weight; see the Red Book (AAP) or UpToDate.com for specific dosing.
Oseltamivir has been studied in children under 1 year, but may not be appropriate for those under one month; consult a pharmacist
Infant 29-60 Days
Pt with h/o prematurity, congenital abnormality presents with sudden onset fever > 38.5 C. Parents report cough, increased WOB, diarrhea with blood/mucus in stool, and treatment with antibiotics during previous 7 days. Tachypnea, grunting, nasal flaring, retractions on exam.
Obtain CBC, BMP, blood culture, U/A with culture
Presenting during influenza season: Obtain influenza PCR
Risk factors for invasive bacterial infection, not currently influenza season, or negative influenza PCR:
Obtain CSF cell count and differential, glucose, and protein
Obtain CSF bacterial culture and enterovirus PCR
Obtain procalcitonin, CRP for risk stratification
Additional tests
Respiratory distress: Obtain CXR
Diarrhea: Obtain stool culture
Treatment
Toxic appearing, ANC < 1,000, PNA on CXR, confirmed UTI, and/or CSF pleocytosis: Admit to hospital and start empiric coverage with cefotaxime
Non-toxic with reliable caregivers: Administer ceftriaxone 50 mg/kg IM and f/u in 24 hours
Concern for Enterococcus and/or Listeria infection: Add ampicillin
CSF positive for S. pneumoniae meningitis: Add vancomycin 15 mg/kg
Positive influenza PCR and within 48h of symptom onset: Start oseltamivir 3 mg/kg/dose BID x 5 days
Supportive care
Maintain adequate hydration
Titrate oxygen to maintain saturations > 92%
Notes
Manage according to adjusted chronological age = (chronological age in weeks - [40 - WGA at birth])
Infections of concern: Respiratory (most common), meningitis (most concerning), UTI
Factors that increase risk for bacterial infection: H/o prematurity/congenital abnormality, comorbid medical conditions, antibiotic therapy within the previous 7 days
U/A is indicated if s/sx of pediatric UTI and/or if respiratory complaints are present. UTI is confirmed with U/A showing positive LE, nitrites, or > 5 WBC/HPF.
Empiric antibiotic doses vary depending on the child's age and weight; see the Red Book (AAP) or UpToDate.com for specific dosing.
While oseltamivir is recommended within 48h of symptom onset, it may reduce morbidity/mortality in children if started later.
Children who do not meet hospitalization criteria (see plan), have confirmed influenza without respiratory distress, or who have confirmed UTI may be discharged to home with appropriate therapy and f/u within 24 hours.
Infant 61-90 Days
Pt with h/o prematurity, congenital abnormality presents with sudden onset fever > 38.5 C. Parents report cough, increased WOB, diarrhea with blood/mucus in stool, and treatment with antibiotics during previous 7 days. Tachypnea, grunting, nasal flaring, retractions on exam.
Labs
Obtain CBC, BMP, blood culture, U/A with culture
Presenting during influenza season: Obtain influenza PCR
Risk factors for invasive bacterial infection, not currently influenza season, or negative influenza PCR:
Obtain CSF cell count and differential, glucose, and protein
Obtain CSF bacterial culture and enterovirus PCR
Obtain procalcitonin, CRP for risk stratification
Additional tests
Respiratory distress: Obtain CXR
Diarrhea: Obtain stool culture
Treatment
Toxic appearing, ANC < 1,000, PNA on CXR, confirmed UTI, and/or CSF pleocytosis: Admit to hospital and start empiric coverage with cefotaxime
Non-toxic with reliable caregivers: Administer ceftriaxone 50 mg/kg IM and f/u in 24 hours
Concern for Enterococcus and/or Listeria infection: Add ampicillin
CSF positive for S. pneumoniae meningitis: Add vancomycin
Positive influenza PCR and within 48h of symptom onset: Start oseltamivir 3 mg/kg/dose BID x 5 days
Supportive care
Maintain adequate hydration
Titrate oxygen to maintain saturations > 92%
Notes
Manage according to adjusted chronological age = (chronological age in weeks - [40 - WGA at birth])
Infections of concern: Respiratory (most common), meningitis (most concerning), UTI
Factors that increase risk for bacterial infection: H/o prematurity/congenital abnormality, comorbid medical conditions, antibiotic therapy within the previous 7 days
U/A is indicated if s/sx of pediatric UTI and/or if respiratory complaints are present. UTI is confirmed with U/A showing positive LE, nitrites, or > 5 WBC/HPF.
Empiric antibiotic dosing depends on the child's age and weight: See the Red Book (AAP) or UpToDate.com for specific dosing.
While oseltamivir is recommended within 48h of symptom onset, it may reduce morbidity/mortality in children if started later.
Children who do not meet hospitalization criteria (see plan), have confirmed influenza without respiratory distress, or who have confirmed UTI may be discharged to home with appropriate therapy and f/u within 24 hours.
Iron Deficiency Anemia
1 y/o with h/o prematurity, immigration from a developing nation presents for fatigue/irritability. Parents report pt regularly tries to eat dirt/clay; deny recent viral illness, rash, joint pain. Growth delay, glossitis, systolic murmur, skin pallor on exam.
Labs
CBC shows low hemoglobin, low MCV, elevated RDW, and reticulocyte count <2%; MCV/RBC > 13
Iron studies show low ferritin, elevated TIBC
Lead level WNL
Start 1 month trial 6 mg/kg iron supplementation to be taken at breakfast; repeat CBC upon completion
Parents advised to limit cow's milk consumption to < 20 ounces per day and supplement diet with iron-rich foods
Notes
Etiology
Insufficient iron intake is the most common reason for childhood anemia; affects 3-10% of children
No recent viral illness/rash/joint pain decreases likelihood of transient anemia due to Parvovirus B19
Labs
Low MCV + elevated RDW indicates iron deficiency
Mentzer index = MCV/RBC count; values > 13 indicate greater likelihood of iron deficiency decreased likelihood of Thalassemia
Reticulocyte count <2% indicates that the anemia is not due to a destructive process
Normal hemoglobin levels are based on age; hemoglobin increase of >1g/dL one month after supplementation confirms diagnosis
Iron supplementation in exclusively breastfed infant:
<37 WGA: Supplement iron (2 mg/kg/day) from 1 to 12 months of age
Full term: Iron supplementation starting at 4 months and continuing until child is eating sufficient iron-containing foods
Lead Toxicity
Pt with h/o immigration from developing nation presents with subacute abdominal pain, irritability, lethargy. Parents report milestone regression and are concerned about possibility of ADHD. Pt lives in house built before 1970. HTN on exam.
CBC shows microcytic anemia; peripheral smear shows basophilic stippling
Obtain serum ferritin, TIBC to r/o iron deficiency anemia
Lead level
5-14 mcg/dL: Repeat lead level to confirm result
15-44 mcg/dL: Obtain abdominal x-ray and perform whole bowel irrigation if suspected lead particles present
45-69 mcg/dL: Repeat level within 48 hours and administer DMSA 10 mg/kg/dose TID x 5 days and then BID x 14 days. Provide nutritional supplementation with MVT with iron and 2 8oz glasses milk.
70 mcg/dL or greater: Emergency consultation advised; contact regional poison control center (1-800-222-1222)
Parents counseled about routes and risks of lead exposure
Parents advised screen all children living in the household for lead
Health department notified
Henoch-Schonlein Purpura (IgA Vasculitis)
5 year old presents with acute onset diffuse/colicky abdominal pain, arthralgias/arthritis, purpura. Symptoms preceded by sore throat. Hypertension and palpable, non-blanching purpura primarily located on lower extremities.

Note: Vasculitis-associated rashes are non-blanching
Labs
CBC may show thrombocytopenia
Obtain initial CMP to evaluate creatinine, serum albumin
Evaluate early morning CMP for creatinine > 30 µmol/L
Obtain PT/PTT/INR
Evaluate urinalysis for proteinuria, hematuria
Consider skin biopsy
Severe abdominal pain: Consider ultrasound to rule out intussusception
Treatment
Continue supportive therapy
Arthritic pain: Acetaminophen per pediatric dosing
Positive strep test and age > 3 years and GFR > 30: Amoxicillin 50 mg/kg qd x 10 days (maximum daily dose 1,000 mg/day)
Renal involvement as evidenced by elevated creatinine, proteinuria, and/or hematuria
Prednisone 1 mg/kg/day x 2 weeks followed by 2 week taper
HTN: Amlodipine 0.1 mg/kg/day (maximum daily dose 5 mg/day)
Consult nephrology
Monitor BP, creatinine, and urinalysis monthly for six months
Refractory abdominal/arthritic pain and/or scrotal swelling: Consider prednisone (see dosing above)
Counseling
Parents informed that 95% of cases resolve spontaneously within 8 weeks
Avoid ibuprofen due to abdominal pain and concern for renal involvement
Relapses can occur for up to 10 years following illness
Notes
Epidemiology
Most common systemic vasculitis of childhood
Typically occurs between age 3-15 years with peak prevalence at age 4-6 years
Only 10% of cases occur in adults
Sometimes associated with preceding streptococcal pharyngitis
Pediatric Rheumatology European Society Criteria
Mandatory: Purpura or petechiae with lower limb predominance
At least one of the following:
Arthritis or arthralgia
Acute onset diffuse abdominal pain
Renal involvement: Proteinuria or hematuria
Histopathology: Leukoclastic vasculitis or proliferative glomerulonephritis with IGA deposits
Treatment
Calcium channel blockers (e.g. amlodipine) are indicated for hypertension associated with renal involvement
Corticosteroids
Prophylactic treatment does not prevent renal disease (SOR A)
Early treatment may reduce joint and abdominal pain