Renal and Genitourinary
Renal and Genitourinary
Young female presents with acute onset dysuria, urinary frequency/urgency. Pt recently became sexually active for the first time. Denies change in urine appearance/odor. Denies chills, rigors, marked increase in fatigue. Denies h/o confirmed multidrug resistant UTI. Afebrile with no suprapubic tenderness on exam; no costovertebral angle tenderness.
Urine dipstick positive for leukocyte esterase, nitrites
Obtain urine pregnancy test, urine culture
Pregnancy test negative: Start nitrofurantoin 100 mg BID x5 days and adjust antibiotic therapy pending culture
Symptom interpretation
Change in urine color/smell is not specific for UTI and should not prompt further workup in the absence of other symptoms
Women who self-diagnose UTI have a 85% positive culture rate; this is more accurate than dipstick testing
Dipstick interpretation
Leukocyte esterase: 75% sensitivity, 98% specificity
Nitrites: 30% sensitivity, 90% specificity
Cranberry products are not effective in relieving symptoms
Pregnancy considerations
Antibiotics
Fosfomycin 3 g as a single dose is safe in all three trimesters, but may have decreased efficacy compared to other first-line agents (IDSA 2018)
Nitrofurantoin is safe in the 2nd and 3rd trimesters
TMP-SMX is contraindicated
Perform test of cure 1 week after starting therapy
Elderly male with h/o indwelling Foley catheter and repeat UTIs presents with new onset urinary frequency/urgency in the setting of increased debility. Caretaker reports recent chills, rigors, flank pain. Fever, altered mental status, abdominal/suprapubic tenderness, costovertebral angle tenderness on exam.
Labs
Obtain CBC, BMP, urine/blood cultures
Dipstick positive for leukocyte esterase, nitrites
Urinalysis positive for pyuria, bacteria
Consider abdominal/pelvic CT with and without contrast in the following scenarios:
Patient meets sepsis criteria
Symptoms do not improve after 72 hours of antibiotic therapy
Admit for inpatient management if the patient meet any of the following criteria:
Debility and/or marked change in overall health status
Fever >38.4
Pt requires IV antibiotic therapy, e.g.
Inability to maintain PO hydration and/or tolerate PO therapy
Treatment with IV agent indicated (see below)
Antibiotic therapy
Meropenem 1 g IV q8 hours x 10 days for any of the following:
History of infection with multidrug-resistant organism
Long term care facility resident or recent hospitalization
Treatment with broad spectrum beta-lactam, TMP-SMX or fluoroquinolone within the past week
Otherwise start ceftriaxone 1 g IV daily x 10 days; transition to cefdinir (Omnicef) 300 mg BID and complete course once pt can tolerate PO intake
Adjust antibiotic therapy pending culture sensitivities
Complicated UTI includes infections extending beyond the bladder, e.g. pyelonephritis
Clinical definition: One of the following must apply
Fever + s/sx systemic illness, e.g. new onset debility, chills/rigors
Pyuria + one of the following
Flank pain/CVA tenderness or imaging indicating pyelonephritis
Fever and/or sepsis
Dipstick interpretation
Leukocyte esterase: 75% sensitivity, 98% specificity
Nitrites: 30% sensitivity, 90% specificity
Microbiology/urine culture
Most commonly associated bacterial pathogens are nitrite producing and include E. coli, Klebsiella, and Proteus species
Positive if >100,000 bacterial colony forming units present
Diagnostic reference: Urinalysis Evidence Based Summary
Young F with h/o sexual intercourse with new male partner, recurrent UTIs, DM presents with urinary frequency/urgency, dysuria, N/V. Pt's mother has h/o recurrent UTIs. T>38 C, CVA tenderness, suprabupic pain on exam.
U/A showing +LE, microscopic pyuria/hematuria; reflex for culture
Obtain BMP; consider ordering lipase, transaminase, beta-hCG
[Pregnent: Admit to hospital and start CTX; transition to oral antibiotics x 10 days once afebrile. Suppressive therapy with daily low-dose nitrofurantoin s/p treatment course.]
Negative urine pregnancy test; start levofloxacin 750 mg BID x 5 days
Re-evaluate pt within 48-72hr
Consider CT if pt's symptoms fail to improve or if symptoms recur s/p initial treatment
Consider hospitalization if pt develops hemodynamic instability, metabolic derangement, severe flank/abdominal pain, toxic appearance, fever or is unable to tolerate PO liquids
Pt with h/o low fluid intake, congenital kidney deformity, primary hyperthyroidism, and DM/gout due to excess sweetened beverage consumption presents with acute onset, paroxysmal flank pain. Flank pain is unilateral and episodes of severe pain generally last 20-60 minutes. ROS positive for N/V, dysuria, and urinary urgency. Reports personal h/o malabsorptive bariatric surgery and family h/o nephrolithiasis. Severe, unilateral CVA tenderness on exam.
Pregnancy test negative
Microscopic hematuria on urinalysis
Low-dose CT with contrast shows hydronephrosis, presence of stone
Stone <10 mm
Administer indomethacin 75 mg BID, tamsulosin 0.4 mg daily, and strain urine with voids
Consult urology if pt requires hospitalization or stone does not pass within 3 weeks in the outpatient setting
Stone >10 mm: Administer ketorolac 15 mg q6 hours and consult urology
Pt advised to keep stone upon passage
Send stone for analysis
Kidney stone types
Calcium stones (80%)
Calcium oxalate: More common and increased risk with malabsorptive bariatric surgery, e.g. Roux-en-Y
Calcium phosphate: Less common than calcium oxalate
Struvite (magnesium ammonium phosphate)
Uric acid
Cysteine
Differential diagnosis to consider
Ruptured aortic aneurysm
Microscopic hematuria may be present
Verify stable BPs to rule out diagnosis
Ectopic pregnancy
Rule out with pregnancy test
Consider pelvic ultrasound if pregnancy test is positive
Other gynecologic issues can also be ruled out with ultrasound, e.g.
Ruptured ovarian cyst
Ovarian torsion
Patient with history of obesity, HTN, and DM type 2 presents with decreased renal function for > 3 months. Decreased urine output, continued unhealthy diet, and progression of diabetic retinopathy on yearly ophthalmologic exam. Denies recent illness, flank pain, pruritic rash. Denies family history of renal disease. HTN with decreased visual acuity on exam. No JVD, M/R/G, abdominal bruit, flank pain, suprapubic tenderness, LE edema, joint swelling/tenderness, rash on exam. Dorsalis pedis pulse 2+ bilaterally.
Labs
Obtain CBC, CMP, lipid panel, HbA1c, urinalysis, urine culture, morning spot urine albumin/creatinine ratio; GFR calculated using National Kidney Foundation (NKF) calculator <60 mL/min/1.73 m^2
Hgb indicates anemia: Obtain reticulocyte count, ferritin level, transferrin saturation, and vitamin B12/folate levels
No urine sediment or casts noted on microscopy
Imaging
Obtain renal ultrasound with Doppler to rule out structural disease, decreased perfusion
Consider nerve conduction study if pt develops paresthesias or s/sx consistent with restless leg syndrome
Blood pressure management per KDIGO for adults with and without DM
Hypertension and not pregnant: Start lisinopril 2.5 (GFR < 30) to 10 mg (GFR > 30) qd for renal protection and titrate to 40 mg daily with close monitoring of serum potassium and creatinine
Albumin-creatinine ratio
< 30 mg/24h: Treat to ≤ 140/90 mmHg
≥ 30 mg/24h: Treat to ≤ 130/80 mmHg with at least one ACE-I or ARB
Monitor for postural hypotension
Treatment per stage (KDIGO recommendations, see notes for shared decision making considerations)
All patient stage ≥ 3a (GFR < 60)
Obtain annual CBC (anemia) and baseline CMP, phosphorous, PTH
Serum bicarbonate < 22 mmol/L: Start oral bicarbonate supplementation
Elevated PTH: Obtain serum 25-hydroxyvitamin D and supplement to > 20 ng/mL
Administer pneumococcal 23 vaccination
Refer to nutrition to discuss caloric, protein, sodium, potassium, and phosphate intake
Stage 3b (GFR 30-44)
Obtain annual CMP, serum phosphate
Do not perform routine bone mineral density testing (risk for misleading results)
Maintain serum phosphate concentrations within normal range
Stage 4 (GFR 15-29)
Obtain CBC every 6 months
Immunize against hepatitis and confirm response with HBV Ab
Do not administer bisphosphonate therapy
Prepare for renal replacement therapy
Stage 5 (GFR < 15): Refer to nephrology for initiation of dialysis
Medication
GFR < 60: Avoid sodium-phosphate bowel preparations
Uremic pruritus: Chronic condition common in advanced CKD. Trial of capsaicin cream and/or mirtazapine.
Refer to nephrology for any of the following:
GFR <30 mL/min/1.73 m^2
Potassium levels persistently > 5.0 meq/L
Two of three early morning spot urine albumin/creatinine ratio > 300 mg/g and spot urine protein/creatinine ratio > 500 mg/g
Development of anemia of chronic disease
Imaging with contrast: Hydrate before/after study and reevaluate GFR within 48-96 hours
Diagnosis
Differential includes alternate etiologies that may be indicated by recent illness, urine sediment/casts on microscopy, etc.
Acute: AKI (Cr 1.5-1.9 x baseline or Cr increase > 0.3 mg/dL), UTI, nephrolithiasis
Chronic: Autoimmune disease, familial kidney disease
Acute or chronic: Medication use, intrinsic renal disease
CKD diagnostic criteria: Must meet one of the following for > 3 months
GFR < 60 ml/min/1.73 m^2
Any marker of kidney damage: Albuminuria ≥ 30 mg/24 hours, electrolyte/urine sediment/structural/histologic abnormality, history of renal transplant
Source: KDIGO Practice Guidelines
Determining Renal Function
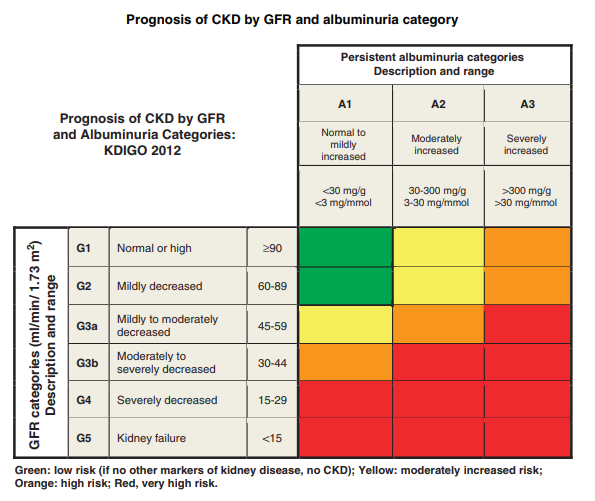
CKD categorized per GFR (see KDIGO chart, NKF calculator) and albuminuria
Creatinine
Creatinine concentrations affected by muscle mass/protein intake and may be less reliable in frail/aging populations
If concern for Cr accuracy, consider cystatin C for confirmation (e.g. GFR 45-59 with no marker of kidney damage)
If GFR per Cr and cystatin C < 60, diagnosis is confirmed
Albuminuria
Term “microalbuminuria” no longer recommended
Spot urine albumin/creatinine ratio (ACR)
Can be collected at any time
Confirm ACR ≥ 30 mg/g with early morning urine sample
Greater values indicate increased risk for progression to ESRD and death
Suspicion for false elevation due to multiple myeloma: Obtain urine kappa/lambda light chain assay (Bence-Jones protein)
Only used for medication adjustments
Calculation becomes increasingly important in elderly patients as GFR declines with age. For example, in two 70 kg male patients with Cr 1:
GFR in the 40 y/o = 44 mL/min
GFR in the 80 y/o = 26 mL/min
Dialysis Considerations
Patients with CKD have variable illness trajectories
Dialysis inconsistently modifies symptoms (i.e. patient dependent)
Mortality is significantly affected by patient characteristics
Average annual mortality for hemodialysis patients is 20%
Dialysis may not prolong survival in the frail/elderly or those with significant comorbidities
Calculators
Elderly male presents with chronic urinary frequency. Reports urgency, weak stream, straining, and nocturia. Denies fever, dysuria, gross hematuria, flank pain. No history of tobacco use, DM, prostate cancer, excessive caffeine intake, or sexual dysfunction. No h/o urologic surgery. Digital rectal exam reveals normal sphincter tone, enlarged prostate, and bladder distention.
Obtain urinalysis
Life expectancy >10 years: Obtain PSA s/p shared decision making
Post void residual showing >100 mL urine
Moderate/severe symptoms and no plans for cataract surgery: Start tamsulosin 0.4 mg daily
Pt encouraged to keep voiding diary between now and next appointment
Pt counseled against using alternative therapies such as saw palmetto
Differential diagnosis
Rule out common causes of neurogenic bladder, e.g. diabetes
Urinalysis
If normal, rules out UTI, nephrolithiasis, bladder cancer
Positive for hematuria in approximately 10% of cases
Alpha blocker (e.g. tamsulosin) are contraindicated in patients undergoing cataract surgery due to risk for intraoperative floppy iris syndrome
Referral for surgery (transurethral resection of the prostate) may be considered for the following:
Symptoms uncontrolled with medical therapy
Development of bladder calculi
Gross and/or microscopic hematuria
Recurrent urinary tract infections
Renal insufficiency
Pt <77 years old with family h/o prostate cancer presents with gradual onset unintentional weight loss, urinary frequency/hesitancy, hematuria, and bony back pain. Denies h/o HTN, chest pain, heart failure, MI, stroke, lung disease, GI ulcer, IBD, DM, depression. Lower extremity weakness and enlarged prostate with asymmetry/nodularity on DRE.
CBC shows anemia
PSA > 10 ng per L indicating intermediate risk or higher; repeat in 1 month for confirmation
Consider monitoring with yearly DRE and PSA every 3 to 6 months
Consider MRI for prostate visualization
Consider referral for 12-core prostate biopsy (sensitivity 80%) to determine Gleason score and quantify disease risk
Treatment per disease risk and Charlson comorbidity index
Low risk disease: Observation vs. active surveillance vs. brachytherapy
Intermediate risk: Treat as low vs. high risk s/p shared decision making
High risk prostate cancer: Consider treatment plan that may include
Androgen deprivation therapy with Lupron (leuprolide) depot 7.5 mg q monthly
External beam radiation therapy (EBRT) vs. radical prostatectomy
Refer to urology
Pt counseled about risks and benefits of observation vs. treatment
Epidemiology
Affects 1 in 7 men
1 in 39 affected men will die from the disease (3rd most common cause of cancer-related death in men)
The reason for the debate about screening:
Treatment may not greatly change the course of the disease and will almost certainly result in undesirable adverse effects.
Patients who present with symptoms as described above (e.g. bony pain and LE weakness due to spinal cord compression) have metastatic disease and will likely not benefit from treatment.
Disease risk
Determined using a Gleason score (requires biopsy) and PSA level
Gleason scores range from 2 to 10
PSA
10 ng per L or greater indicates intermediate risk or higher
20 ng per L or greater indicates high risk
Adjusted life expectancy
Performed using Charlson Comorbidity Index with 1 point each for the following: HTN, chest pain, heart failure, MI, stroke, lung disease, GI ulcer, IBD, DM, depression
Do not treat very low or low risk patients if
62+ years old with 3 or more comorbidities
77+ years old with any comorbidities
Observation/treatment modalities
PSA rise >0.75 ng/dL in one year is concerning
Brachytherapy: Implanted radioisotopes (fewer adverse effects)
EBRT: Precision radiation of prostate (risk for urinary incontinence, erectile dysfunction, scarring of urethra/GI tract)
Radical prostatectomy: Removal of prostate that limits disease progression (almost certain urinary incontinence, ED)

Prostate cancer staging
Male hairdresser age >35 years with h/o chronic UTI, pelvic radiation, smoking, and NSAID analgesic abuse presents with asymptomatic hematuria. No pertinent positive on ROS. No abnormalities on physical exam.
Obtain BMP
Urinalysis shows gross hematuria
Obtain CT to evaluate upper urinary tract
Imaging
Refer to urology for cystoscopy
Cystoscopy negative with risk factors for malignancy: Obtain CT abdomen/pelvis with and without contrast
Lesions suspicious for malignancy on imaging: Refer to oncology
Pt counseled about risks of smoking, analgesic abuse
Epidemiology
Responsible for 5% of asymptomatic hematuria cases
Occupational exposure to benzenes or aromatic amines (e.g. hairdressers) increases risk
May present with gross or microscopic hematuria
Pt age >75 years with h/o cardiovascular disease, heart failure, alcoholism presents with new onset incontinence, urinary frequency, and nocturia. Episodes preceded by intense desire to urinate and pt often loses control of bladder en route to bathroom; this is followed by large volume urine loss. Mediations include diuretics. Minimal, delayed leakage following cough stress test.
Variable volume loss noted on 3 day voiding diary
Obtain urinalysis with reflex microscopy and urine culture
Post void residual <50 mL
Comorbid condition management
Vaginal atrophy present: Start intravaginal estrogen therapy
Pt advised to reduce alcohol consumption
Initial therapy
Start 3 daily sets of 8 to 12 pelvic floor contractions sustained for 8 to 10 seconds each
Start bladder training with timed daily voids occuring at the shortest interval indicated on the 3 day voiding diary
Control urgency between voids with relaxation techniques, e.g. deep breathing
Increase interval between voids by 15 minutes following each day without incontinence
Goal: Timed voids every 3-4 hours
Failure of initial therapy
Trial of mirabegron 25 mg once daily x8 weeks
Mirabegron not covered by insurance and no contraindication to anticholinergic therapy: Start one of the following
Oxybutynin immediate-release 5 mg TID
Trospium chloride (Sanctura) 20 mg BID
Consider referral to pelvic PT
Consider referral to urology
Present in ~10% of women age 40-45 years
Present in >30% of men and women age >75 years
Potential etiologies
Detrusor instability: Detrusor overactivity or loss of inhibitory control of bladder contractions
Sensory: Urge to urinate caused by local irritation, inflammation, or infection
Contraindications to anticholinergic
40 year old F with h/o chronic cough, grand multiparity presents with chronic, small volume urine loss. Urine loss typically occurs when coughing, sneezing, jumping, lifting, or exercising. Episodes have even occured with minimal activity, e.g. rising from chair. Denies nocturia. Medications include alpha-adrenergic agonists and ACE inhibitor. Positive cough stress test on exam.
Small volume leakage (<10 mL) on 3 day voiding diary
Obtain urinalysis with reflex microscopy and urine culture
Post-void residual <50 mL
Initial therapy
Refer for pessary fitting
Consider referral to pelvic PT
Consider duloxetine 20 mg twice daily for 2 weeks then 40 mg BID in patients with comorbid depression
Failure of initial therapy: Refer for surgical evaluation for mid-urethral sling placement
Epidemiology
Present in 30% of women age >30 years
May occur in men s/p prostate surgery
Etiology: Sphincter and/or pelvic floor weakness
Cough stress test
Most reliable clinical assessment for stress incontinence
Positive if small volume leakage occurs with cough and stops once coughing terminates
Negative if no leakage occurs or if leakage occurs >5 seconds after coughing terminates
Pelvic floor exercises: 3 daily sets of 8 to 12 pelvic floor contractions sustained for 8 to 10 seconds each
Do NOT refer for urodynamic testing
Elderly M pt with h/o BPH, DM, multiple sclerosis and alcoholism presents with chronic incontinence. Reports inability to empty bladder, dribbling, hesitancy, and urine loss without sensation of fullness/pressure in lower abdomen. Medications include calcium channel blockers, opioids, muscle relaxants, antidepressants, antiparkinsonian agents, sedatives, and anticholinergics. Bladder distention, peripheral neuropathy, decreased sphincter tone, and enlarged prostate on exam; no leakage noted on cough stress test.
No consistent pattern noted in 3 day voiding diary
Obtain urinalysis with reflex microscopy and urine culture
BMP shows increased serum creatinine
Post void residual >200 mL
Treatment in men
Pt avoid to lose weight and perform daily pelvic floor muscle exercises
Start tamsulosin (Flomax) 0.4 mg daily and increase to 0.8 mg daily after 4 weeks
Concern for prostate cancer or failure of initial treatment: Refer to urology
Pt advised to decrease alcohol intake and adhere to prescribed DM regimen
Leakage is caused by bladder overdistention
DM and alcoholism
Resulting peripheral neuropathy can lead to overflow incontinence
May be indicated by peripheral neuropathy or decreased anal sphincter tone on exam
Elderly pt with h/o cognitive impairment due to CVA/dementia and decreased mobility due to arthritis presents with chronic incontinence. Caregiver reports variable urine leakage, difficulty transporting patient to and from bathroom. Medications include COX-2 selective NSAIDs, sedative-hypnotics, and thiazolidinediones. Negative cough stress test.
MOCA <26
<50 mL on post-void residual
Caregiver counseled that incontinence is most likely related to delayed transport time to toilet and not a physiologic mechanism
Pt with h/o ESRD presents with BUN >60 mg/dL. Reports confusion, fatigue, anorexia, vision loss, chest pain, N/V, erectile dysfunction, decreased libido, pruritus, LE numbness/tingling, seizures. Medications include diuretics, NSAID, ACE inhibitor, macrolide antibiotic. Fever, orthostatic hypotension, PERRLA, dry mucous membranes, pleuritic chest pain, pericardial friction rub on exam.
Obtain CBC, CMP, PT/PTT/INR, ABG, urinalysis with microscopy
Albumin:creatinine ratio >300 mg/g
RBC casts on urine microscopy
EKG shows no diffuse ST or T-wave elevations
Treatment
Administer 1L bolus NS and re-evaluate volume status
Stop diuretics, NSAID, ACE inhibitors; transition to alternative antibiotic regimen
Pt actively bleeding; consider desmopressin, cryoprecipitate, estrogen, and/or dialysis to improve platelet function
Place hemodialysis catheter and initiate emergent hemodialysis
Pt will require long-term renal replacement therapy; discuss hemodialysis versus peritoneal dialysis
Consults
Consult surgery about placement of AV fistula vs. peritoneal dialysis catheter pending pt preference
Consult nephrology
Pt educated about s/sx of uremia
Hypovolemia is a common cause of transient declines in kidney function
Decreased glomerular filtration: NSAIDs prevent afferent arteriole dilation and ACE inhibitors prevent efferent arteriole constriction
Aminoglycoside (e.g. gentamicin, tobramycin, neomycin) toxicity may precipitate uremia
Uremia impairs platelet function and increases bleeding risk
Uremic pericarditis presents as fever, pleuritic chest pain, friction rub. Unlike other pericarditis etiologies, there is no ST or T-wave elevation on EKG.
AV fistulas are used for hemodialysis 2-5x per week and require at least 1 month to mature
Uremic neuropathy is characterized by LE numbness/burning and may be a contraindication to initiating dialysis
Severe uremia may cause transient cortical blindness