Musculoskeletal

Musculoskeletal
Clavicle
Acromioclavicular injury
Clavicle fracture
Glenohumeral dislocation (most common dislocation)
Proximal humerus fracture
Young adult presents with shoulder pain after falling onto shoulder while being tackled during a football game. Patient was carrying the football and suffered medial/inferior joint stress at the time of the injury. No swelling, deformity of clavicle with a negative cross body adduction test. Active and passive shoulder range of motion intact. Full strength with shoulder abduction, adduction, extension and flexion. Radial pulses 2+, capillary refill < 2 seconds, and no skin discoloration bilaterally. Sensation normal in shoulders, arms, and hands bilaterally.
Obtain anteroposterior view, Zanca view, axillary x-rays of clavicle
Treatment
Pain management: Acetaminophen, ibuprofen (age/weight based dosing)
Management per clavicle elevation (see below)
Clavicle elevation and injury classification (Rockwood system)
< 25%
Discontinue shoulder sling once symptoms are tolerable with pain management alone
Encourage range of motion exercises
Refer to physical therapy
Patient counseled that pain may last up to 6 weeks
≥ 25%
Refer to orthopedics
Patient counseled that pain may last for 3 months
Patient counseled that he is at increased risk for future AC joint arthritis and/or degenerative changes
A football player for a Charlotte-based professional football team sustains a shoulder injury while performing a “superman” dive into the endzone. Player reports he landed on the anterior aspect of his shoulder during the descent. Denies shortness of breath. Radial pulses 2+ and capillary refill < 2 seconds. Patient able to touch thumb to each finger and spread fingers against resistance. Sensation intact in shoulders/arms/hands bilaterally.
Obtain x-ray of affected clavicle
Treatment
Refer to orthopedics if any of the following are present: Open injury, skin tenting, displaced group 1, any group 2 injury
Orthopedic referral not required
Place arm in sling during day for 2 to six weeks
Refer to physical therapy
Patient instructed to present to the emergency department immediately if he develops dyspnea or severe unilateral paresthesias
Follow-up for re-evaluation in 4 weeks
Notes
Grouping system determines risk for brachial plexus injuries
Group 1 = proximal 3rd of clavicle
Group 2 = distal 3rd of clavicle
Group 3 = middle third of clavicle
Ask about shortness of breath to rule out pneumothorax
Young adult patient with h/o glenohumeral instability, shoulder dislocation/subluxation, and participation in overhead sports present with acute onset shoulder pain s/p fall from bicycle. Reports lateral arm numbness. Patient noted to be holding affected arm in contralateral hand. Palpable humeral head in axilla, dimpling inferior to acromion, reduced range of motion, and lateral arm numbness on exam.
Imaging
Obtain AP, scapular Y, and axillary x-ray to r/o fracture and to confirm successful reduction (see treatment)
Concern for axillary nerve injury due to lateral arm numbness, neurovascular deficits: Obtain baseline EMG
Treatment
Injection and reduction
Prepare 20 mL intra-articular lidocaine 1% without epinephrine
Inject 1.5 cm distal and 2 cm medial to posterolateral corner of acromion
Reduce shoulder and repeat radiographs to confirm success
Instruct patient to wear sling x 4 weeks
Follow-up 2 weeks s/p injury
No pathology on initial plain films: Repeat AP, scapular Y, and axillary views
repeat EMG if no significant improvement has occured
Encourage early mobilization to prevent frozen shoulder
Consults
Recurrent dislocation: Refer to orthopedics for evaluation
Elite athlete: Consider orthopedics referral due to high risk for repeat dislocation
Patient counseled that repeat dislocation risk increases with age and each repeat injury
Elderly patient with h/o osteoporosis presents with acute shoulder/upper arm pain following a fall from standing position. Radial pulses and 2+ capillary refill bilaterally. Sensation present over lateral deltoid and in the medial, ulnar, and radial nerve distributions of the hand on the affected arm.
Imaging
Obtain anteroposterior view of glenoid, scapular Y view, axillary view
If imaging is normal, repeat radiographs at 3 weeks to rule out occult fracture
Treatment
Non-displaced fracture
Non-operative management recommended as it provides better outcomes
Apply sling x 6 weeks and then start range of motion exercises
Displaced fracture and/or cool, pulseless extremity: Refer to orthopedics for evaluation
Pt with h/o shoulder dislocation/subluxation presents with shoulder pain s/p collision sustained while playing an overhead sport. Reports numbness over lateral deltoid. Generalized ligamentous laxity, positive apprehension test and joint relocation on exam.
Consider shoulder x-ray; evaluate for Hill-Sachs lesion, dislocation, and inferior glenoid avulsion fracture
Refer to PT for strength training
Consider surgery if recurrent dislocation/subluxation occurs
Pt presents with shoulder pain worse with overhead activity. Exam reveals subacromial tenderness, restricted ROM, pain with abduction/external rotation. Positive Neer, Hawkins test.
Obtain shoulder x-ray; consider MRI
Start Tylenol/NSAIDs for pain and refer to PT; refer to orthopedics if no improvement in 6-12 weeks
Consider corticosteroid injection for temporary relief
Severe pain and significant weakness on exam: Refer to orthopedics
Pt advised to avoid overhead activity

Supraspinatus. Source: Anatomography: CC BY-SA 2.1 jp.
Pt age > 40 y/o with h/o shoulder trauma presents with diffuse shoulder pain. Pain present at night and worse with overhead activity. Exam reveals muscle atrophy and pain with empty can test, Neer test, and Hawkins-Kennedy tests. Weakness noted with external rotation, internal rotation, and Gerber lift-off test.
Diagnosis per physical exam
Positive empty can, Hawkins-Kennedy test: Supraspinatus injury
Positive Neer test: Subacromial impingement syndrome
External rotation weakness: Infraspinatus vs. teres minor injury
Internal rotation weakness and positive lift-off test: Subscapularis tear
X-ray shows superior humeral head migration/sclerosis, loss of acromial-humeral interval
Imaging
Consider MRI
Consider U/S vs. CT arthrography if MRI contraindicated
Start Tylenol/NSAIDs for pain and refer to physical therapy
Refer refer to orthopedics if
No improvement after 6-12 weeks of physical therapy
Severe pain and significant weakness on initial exam
Pt advised to avoid overhead activity

Infraspinatus. Source: Anatomography: CC BY-SA 2.1 jp.

Teres minor. Source: Anatomography: CC BY-SA 2.1 jp.

Subscapularis. Source: Anatomography: CC BY-SA 2.1 jp.
Note: If the initial exam is concerning enough to warrant MRI, the patient should be referred to orthopedics where an MRI will likely be performed. (In other words, MRIs are rarely ordered by primary care physicians in areas with reasonable access to specialists.)
Pt > age 40 with h/o DM, thyroid d/o, previous shoulder surgery presents with diffuse shoulder pain. Gradual onset of pain and stiffness, pain present at night. Decreased active/passive ROM in all planes, pain with movement on exam.
Obtain HbA1c, TSH, free T4
Consider shoulder x-ray
Refer to PT and start acetaminophen vs NSAID
Consider intra-articular corticosteroid injection
Refer to orthopedics if no improvement in 6-12 weeks
Pt advised that condition will most likely resolve spontaneously within 1-2 years
Pt with h/o trauma presents with anterior/superior shoulder pain. Acromioclavicular joint tenderness, painful cross-body adduction test on exam.

Shoulder joint, posterior view. By Jmarchn - Own work.
Obtain shoulder x-ray
Start Tylenol/NSAIDs, heat, and stretching for pain
Consider intra-articular corticosteroid injection vs. surgery if symptoms do not improve
Patient age > 50 years with h/o autoimmune disease/arthritis, shoulder injury, and previous shoulder surgery presents with progressive, diffuse shoulder pain in deltoid region. Reports gradual onset of shoulder stiffness and loss of motion due to pain with activity. Sometimes experiences pain at night on the affected side. Joint line tenderness under the coracoid process, crepitus with active/passive range of motion, restricted external rotation, weakness with overhead arm raise, and a positive Apley scratch test on exam.
Obtain shoulder x-ray and evaluate for joint space narrowing, spurring/osteophytes
Conservative therapy
Start Tylenol/NSAIDs, heat, and stretching for pain
Refer for 6 week course of physical therapy
Patient advised to avoid overhead activity
Follow up in 6 weeks
Additional treatment
No improvement after 6 weeks: Inject glenohumeral joint with mixture of
1 mL triamcinolone acetonide 40 mg/mL
2 mL 1% lidocaine without epinephrine
No improvement at 3 months
Consider repeating radiographs to evaluate for disease progression
Schedule repeat joint injection 3 months after initial injection
Refer to orthopedics for persistent pain affecting quality of life and no improvement after 3 months of conservative therapy and 2 shoulder injections at least 3 months apart; patient counseled that treatment options may include
Osteophyte debridement in patients younger than 50 years
Prosthetic joint replacement
Patient counseled that the results of shoulder surgery are variable and that symptoms generally recur to some degree within 10 years of the procedure
Overall, glenohumeral osteoarthritis an uncommon cause of shoulder pain
Generally preceded by remote history of shoulder injury

Non-septic olecranon bursitis. Soure: NJC123.
50 y/o plumber with h/o alcoholism, immunocompromised state, DM and end-stage renal disease on hemodialysis presents with acute onset, mildly tender unilateral elbow swelling after repeatedly striking the affected elbow against pipes while working. Pt can expel serous fluid from lesion with minimal manipulation, but swelling returns within a few hours. Denies fever, chills. Denies personal, family history of rheumatologic disease and/or gout. Bursal enlargement with mild tenderness and surrounding edema noted on exam. Decreased ROM due to swelling, but not pain.

Prepatellar bursitis. Source Atropos235 - Own work
Presentation is similar to olecranon bursitis, but microtrauma is due to frequent kneeling/crawling. Associated professions/activities include plumbers, roofers, wrestling, and gardening.
Significant bursal enlargement
Imaging
Ultrasound shows enlarged bursa, thickened bursal sac
Color Doppler negative for hyperemia
Recent trauma or concern for foreign body: Obtain plain radiography
Initial management
Rest, ice, and elevation to resolve acute swelling
Naproxen 500 mg BID for swelling and pain
Elbow padding to reduce future trauma
If swelling persists or is bothersome to the patient, consider intralesional corticosteroid injection vs. referral to orthopedics for surgical bursectomy
Pt instructed to contact provider if s/sx of septic bursitis develop (see below)
Pt returns with increased pain and decreased ROM at the bursitis-affected elbow. Reports skin trauma at bursa site due to repeat attempts to aspirate sac at home. Fever, erythema, surrounding edema, and tenderness to palpation noted on exam. Temperature of skin overlying bursitis 2°C greater as compared to non-affected elbow.
Obtain CBC, CMP, ESR, CRP, and blood culture
Cloudy/purulent aspirate shows > 1,500 WBC/mm^3, fluid:serum glucose < 0.5, positive Gram stain, no crystals; f/u culture results
Start cephalexin 500 mg q6h x 10 days and adjust therapy pending culture
Imaging
Ultrasound shows enlarged bursa +/- surrounding cellulitis
Hyperemia on color Doppler indicating infection
Bursa aspiration unsuccessful: Obtain MRI
Failed outpatient management and/or concern for systemic infection: Admit to hospital, start vancomycin, and consult orthopedics
Differential diagnosis includes rheumatoid arthritis and gout
Olecranon bursitis
Most common in patients with repeat elbow microtrauma, e.g. students, draftsmen, plumbers, technicians, and miners
Increased prevalence in hemodialysis patients; the pathophysiology responsible for this association is unknown
Septic bursitis
80-85% of cases associated with S. aureus
Risk factors
Patients with h/o alcoholism, immunocompromised state, DM, and ESRD
Skin injury at or near bursa site
Repeat attempts to aspirate bursa at home
Pregnant, early middle-aged female with h/o obesity, DM, hypothyroidism, rheumatoid arthritis presents with pain and paresthesias in distribution of median nerve. Pain often awakens patient from sleep and is reduced by shaking hand (flick sign). Square shaped-wrist with loss of two-point discrimination, positive Phalen/Tinnel/median nerve compression tests on exam.
Obtain HbA1c, TSH
Consider obtaining rheumatoid factor, anti-CCP antibodies
Ultrasound showing median nerve cross-sectional area < 9mm
Treatment
Consider median nerve glide exercises, yoga
Start neutral wrist splint
No improvement after 6 weeks of conservative therapy
Consider prednisone 20 mg x 10 days
Consider 80 mg methylprednisolone local injection
Failure of conservative management after 4-6 months: Refer for nerve conduction studies/needle electromyography and consider surgical intervention
More common in women
Flick sign
Patient experiences relief s/p shaking hand
93% sensitive and 96% specific for carpal tunnel syndrome
Pathophysiology and physical exam
Median nerve distribution: Palmar aspect of thumb/index/middle fingers and radial half of ring finger
Sensory nerves are more susceptible to compression that motor nerve fibers
Two point discrimination: Inability to distinguish between points less than 6 mm apart
Treatment
Ineffective therapies: NSAIDs, vitamin B6
Oral corticosteroids can improve pain for up to 8 weeks
Corticosteroid injection
Can reduce pain for 1 month and delay need for surgery at 1 year
Risks include median nerve injury and tendon rupture
35 y/o F with no h/o trauma presents with insidious onset wrist pain. Pain worse with gripping/grasping objects and picking up her 6 month old child. Pain is affecting her work as a calligrapher. Mild wrist swelling with tenderness upon palpation of radial styloid/anatomic snuff box, positive Finkelstein test, and negative grind test on exam.
Pain relief with diagnostic lidocaine injection of first extensor compartment
Treatment
Naproxen 500 mg BID
Mild case: Thumb spica splint for pain relief
Moderate to sever case: Administer glucocorticoid injection

Thumb spica splint
Most common in females age 30-50 years
Inciting factors may include picking up a child or occupations that include prolonged gripping/grasping
Pathophysiology: Inflammation of the extensor pollicis brevis and abductor pollicis longus tendons that form the border of the anatomic snuff box
Diagnosis
Arm is held with elbow at approximately 90 degrees with the radial aspect of the wrist superior. A fist is made with the fingers covering the thumb and the hand is flexed inferiorly at the wrist.
Good sensitivity and specificity
Grind test: Pressure is placed on the DIP of the thumb as it is rotated; a positive test would suggest basal thumb arthritis instead of de Quervain's tenosynovitis
Consider obtaining CBC, CRP, ESR if suspicious for infectious tenosynovitis
Pain relief with lidocaine rules out arthritic cause
Persistent inflammation may produce stenosing tenosynovitis
70 y/o F with h/o osteoporosis presents with acute onset wrist pain s/p fall on outstretched hand (FOOSH). Denies h/o peripheral vascular disease, previous wrist injury/surgery. Wrist swelling, but no open fracture/deformity or pain with palpation of anatomic snuff box. Appropriate capillary refill; motor/sensory function intact in region of median, radial, and ulnar nerves.
Postero-anterior (PA), lateral, and oblique wrist views reveal distal radial fracture
Pain control
Opiate naive: Administer 1 time dose 2.5 mg morphine IV if necessary
Calculated CrCl ≥ 30 mL/minute: Start naproxen 500 mg BID
Apply sugar-tong splint allowing for full MCP flexion/extension
Counseling
Pt instructed to elevate arm and apply ice to affected extremity
Pt encouraged to perform shoulder and finger range of motion exercises
Pt advised to seek medication attention if widespread discoloration or numbness/tingling develop in affected extremity
Follow-up outpatient with orthopedics
Pain with palpation of anatomic snuff box should raise suspicion for scaphoid fracture
Obtain emergent orthopedic consult for
Open fractures
Development of neuropathy/vascular compromise
Pt presents with acute onset pain at distal interphalangeal (DIP) joint after being struck by a basketball with finger in full extension. Injury occurred within the previous 3 months. Dorsal DIP tenderness with no active DIP extension when isolated during exam.

Mallet finger injury. Source: Clappstar.

Mallet finger mechanism of action. Source: Davplast.
Imaging
Initial 3-view radiography (anteroposterior, true lateral, and oblique views) shows bone fragment on dorsal surface of proximal distal phalanx
3-view radiography s/p splinting shows confirms alignment of fracture fragment
Intervention
Continuously splint in extension DIP x 8 weeks
Unable to perform full passive extension and/or avulsion fracture involving > 30% of the joint: Refer to orthopedics
Counseling
Pt counseled that failure to adhere to splinting recommendations and not to flex joint during treatment as it could result in permanent injury
Pt reassured that athletic activities that do not place joint at risk of re-injury may continue during splinting
Pt instructed to contact provider if distal phalanx blanching is noted during splint as reduced blood supply can result in distal finger necrosis
Notes
Most common tendon injury of the hand
Can be treated for up to 3 months s/p injury
Passive extension is performed by examiner
Patient adherence to splinting determines treatment success
See link for more information and images
Pt presents with acute onset pain at the distal interphalangeal (DIP) joint after grabbing an opponent’s jersey during a game. Per description, mechanism of injury resulted in forceful hyperextension of DIP. Volar DIP joint tenderness and inability to actively flex DIP when isolated.
3-view radiography shows bone fragment at volar surface of proximal distal phalanx
Finger splinted and patient urgently referred to hand surgeon due to risk for tendon retraction
Pt advised that surgery may be required within 7-10 days to prevent permanent injury
Mnemonic device: The term ‘Jersey Finger’ also describes Garden State residents’ inability to perform active finger flexion while driving
Pt with presents with acute onset thumb pain that occured when s/p falling while holding a ski pole. Per description, mechanism of injury resulted in forced abduction and hyperextension of metacarpophalangeal joint. Exam reveals swelling and tenderness along ulnar aspect of thumb, inability to form a pinch grip with thumb and index finger.
Recall correct anatomic position when describing the hand. Source: Connexions
Obtain 3-view radiography of thumb
Intervention
Stable joint: Immobilize with thumb-spica splint x 4 weeks; refer to orthopedics for instability persisting s/p splinting
Refer to orthopedics in cases of
Pediatric patient
Instability with MCP flexion when finger held at 30 degrees of flexion
Pt advised to avoid heavy gripping or grasping until hand strength returns to baseline
Note: Ulnar collateral ligament injuries are knows as skier’s or gamekeeper’s thumb as they are commonly occur with repeat force applied by ski poles or breaking the necks of small animals (e.g. pheasants, rabbits)
Pt with no h/o osteoporosis, osteoarthritis, malignancy presents with low back pain. Denies fever, weight loss, morning stiffness, gynecologic symptoms, urinary/GI problems. Negative straight leg raise on exam, 2+ reflexes and 5/5 LE strength b/l.
Initial management
Review/establish reasonable goals for pain control
Apply superficial heat
Obtain CMP prior to starting standing NSAID, Tylenol if concern for renal/hepatic dysfunction
Start naproxen 500 mg BID
Start Tylenol 500 mg 4 times daily PRN x 6 weeks
Consider cyclobenzaprine immediate release 5 mg TID x 2 weeks
Refer to physical therapy x 6 weeks (moderate quality evidence)
Follow-up at 6 weeks: If pt has not achieved reasonable pain control goals
Consider acupuncture (moderate quality evidence)
NSAIDs ineffective, consider alternative therapies for chronic back pain (low quality evidence):
Duloxetine 30 mg qd for 1 week then increase to 60 mg qd as tolerated
Tramadol ER 100 mg qd then increase daily dose by 100 mg per week to maximum of 300 mg qd
Consider lumbar spine radiography in 1-2 months and/or referral to orthopedics vs. pain management
Counseling
Pt advised to remain active and engage in low-impact exercise (moderate quality evidence)
Pt counseled about realistic expectations for pain relief
Pt with no h/o recent trauma presents acute onset back pain. Describes sharp/shooting low back pain with unilateral lower extremity radiation in a dermatomal distribution. Denies red flag symptoms including fevers, chills, night sweats, unexplained weight loss, leg weakness, urinary retention, fecal incontinence. Denies h/o vertebral fracture, malignancy, HIV, IV drug abuse. Positive straight leg raise, no lower extremity strength/sensory deficits, and no hyperreflexia with patellar/achilles reflexes on exam.
Initial treatment
Obtain CMP prior to starting standing NSAID, Tylenol if concern for renal/hepatic dysfunction
Start naproxen 500 mg BID
Start Tylenol 500 mg 4 times daily PRN x 6 weeks
Refer to physical therapy
Pt instructed to call office if any red flag symptoms develop (see HPI)
Schedule follow-up visit at 6 weeks
If NSAIDs ineffective consider
Amitriptyline 50 mg qhs; titrate to 150 mg qhs as tolerated
Gabapentin immediate release 100 mg qhs; increase daily dose by 100 mg per week to 100 mg TID (maximum daily dose 1,200 mg TID)
Continued pain/radicular symptoms and/or new onset disability
Obtain MRI
Refer to orthopedics for epidural steroid injection
Notes
Most common etiologies include nerve root compression associated with
Disc herniation
Spondylosis (neural foraminal stenosis generally due to degenerative arthritis)
Nonskeletal etiologies include acute infection, vascular disease, and/or neoplasm
Pt with no significant PMH presents with back pain. Reports progressive motor/sensory deficit, bilateral sciatica, leg weakness, difficulty urinating, and fecal incontinence. Saddle anesthesia on exam.
Emergent MRI consistent with spinal cord compression
Concern for neoplastic epidural spinal cord compression
Refer for emergent surgery to be performed within 24 hours
Start dexamethasone
Day 1: 10 mg IV followed
Day 2 until surgery: Continue dexamethasone 8 mg PO BID
S/p surgery: Taper total dexamethasone dose by half every three days
Note: Urinary retention has 90% sensitivity for this condition; the probability of cauda equina in the absence of urinary retention is 1 in 10,000
Pt age >50 y/o with h/o osteoporosis, chronic oral steroid use, and IV drug use presents with chronic back pain. Reports recent trauma. Pain with palpation on exam.
Obtain CBC, ESR, CRP
Obtain plain radiography
Consider MRI if initial testing negative and pain persists
Pt advised to seek emergency treatment for new onset neurologic disability
Pt with h/o immunosuppression, IV drug use, and recent UTI presents with back pain with no improvement s/p 6 weeks conservative therapy. Reports fever, chills, peri-spinal penetrating wound. Fever, pain with palpation of back on exam.
Obtain CBC, ESR, CRP
Obtain plain radiography
Consider referral for emergency treatment
Pt age >50 y/o with h/o cancer presents with chronic back pain with no improvement s/p six weeks conservative therapy. Reports unrelenting pain at night, progressive motor/sensory deficits, unexplained weight loss. Pain with palpation on exam.
Obtain CBC, ESR, CRP
Obtain plain radiography
Consider emergent MRI due to progressive motor/sensory deficits
Pt advised to seek emergency treatment for unexplained fever, new onset neurologic disability
Young male pt with h/o acute anterior uveitis, aortic regurgitation, restrictive lung disease, IgA nephropathy presents with low back pain/stiffness for > 3 months. Pain improves with exercise/activity. Decreased chest expansion and reduced range of lumbar spine forward flexion on Schober testing.
Evidence of sacroiliitis on anteroposterior and lateral x-ray
Obtain HLA B27 assay
X-ray of anteroposterior/lateral lumbar spine, lateral c-spine, and pelvis in 3 months to monitor disease progression
Start NSAIDs
Pt advised to engage in regular aerobic exercise
Elderly female with history of osteoporosis, multiple myeloma presents with acute onset midline back pain status post fall. Reports recent coughing, heavy lifting prior to injury. No sensory deficits, focal weakness, clonus on exam.
Obtain CBC, CMP, 25-hydroxyvitamin D
Consider MRI if focal neurologic deficits develop
Schedule DEXA scan to assess future fracture risk
Pain management
Acetaminophen, ibuprofen
Administer intranasal calcitonin 200 units (1 spray) in one nostril once daily x 4 weeks
Consider tramadol 50 mg q6h for additional pain control
DEXA scan T-score indicating osteoporosis:
Start alendronate 70 mg once weekly
Patient advised to take alendronate in the morning and remain upright for ≥ 30 minutes before any additional PO intake, including medications
Risk factors
Medical conditions: Osteoporosis, multiple myeloma
Fracture generally occurs following coughing, heavy lifting, or fall
Evaluation
Obtain testosterone levels for compression fractures that occur in men
MRI indicated for neurologic deficits, e.g. sensory deficits, focal weakness, clonus
Treatment
Calcitonin treats short term pain, i.e. < 4 weeks
Bisphosphonates (e.g. alendronate) treat osteoporosis and prevent recurrent fractures
Weak evidence for kyphoplasty
Strong evidence against vertebroplasty
Postmenopausal white female > 40 y/o with presents for follow-up status post hip fracture. Reports sedentary lifestyle, poor diet, active smoking status, consuming > 2 alcoholic drinks daily. Medications include chronic glucocorticoids. Mother suffered hip fracture. Low BMI on exam.
Obtain CMP, TSH, and 25-hydroxyvitamin D
Obtain DEXA for any of the following:
Age ≥ 65 years with no previous DEXA
FRAX calculation indicates 10-year risk > 8.5% risk for major osteoporotic fracture and > 1.0% for hip fracture: Refer for DEXA scan
DEXA scan shows bone mineral density (BMD) ≤ 2.5: Start treatment
No esophageal abnormalities: Alendronate 35 mg weekly x 5 years
Patient counseled to take medication with water only and remain upright for 30 minutes afterward
Discussed small, but potential risk for jaw osteonecrosis/fracture
Bisphosphonates (e.g. alendronate) contraindicated
Obtain CMP: Verify creatinine clearance ≥ 35 mL/min and no hypocalcemia
Start zoledronic acid 4 mg IV every 4 weeks
Consider
Vitamin D 800 IU daily
Intranasal calcitonin x 4 weeks for vertebral compression fracture pain
Counseling
Stop smoking, consume 7 or fewer alcoholic drinks/week (females), and reduce caffeine consumption to ≤ 2.5 cups of coffee daily
Exercise to maintain bone mineral density
Fall prevention
Epidemiology
Fifty percent and 20% of white women and men, respectively, will suffer an osteoporosis-related fracture
20% require long-term nursing care
10% mortality rate
Risk factors include: Postmenopausal state, parental history of hip fracture, smoking, excessive alcohol consumption, low body weight, previous fracture/fall within the past year
Secondary causes of osteoporosis: Primary hyperthyroidism, vitamin D deficiency, chronic glucocorticoid use (≥ 5 mg prednisone daily for ≥ 3 months)
Risk assessment
FRAX tool: Calculates 10 year risk for major osteoporotic and hip fractures for men and women
Average 10-year risk for 65 y/o white woman with no other risk factors:
Major osteoporotic fracture ~8.5%
Hip fracture ~1.0%
DEXA scan screening
All women age ≥ 65 years
Women age < 65 years with fracture risk ≥ average risk for a 65 y/o white woman (8.5%) with no additional risk factors
Osteoporosis z-score (standard deviation)
Defined in relation to the young adult female mean (z = 0)
Osteoporosis defined as z ≤ 2.5 (consider bisphosphonate therapy)
Do not repeat for at least 2-3 years
Therapy
Start bisphosphonates per National Osteoporosis Foundation criteria, i.e. one of the following:
DEXA score ≤ 2.5 and FRAX ≥ 20%
Hip fracture risk ≥ 3%
Second line medications for women who cannot take bisphosphonates include teriparatide and raloxifene
Elderly F pt h/o obesity, knee injury presents with chronic knee pain. Reports joint pain that is worse with movement and affects activities of daily living. Denies h/o gastric ulcers, GI bleeding. Family h/o knee osteoarthritis. Joint effusion, valgus/varus deformity, lateral instability, and pain/crepitus with passive ROM on exam.
Obtain baseline BMP
Knee x-ray shows joint space narrowing, sclerosis, and osteophytosis
Initial treatment
Regular icing for improved range of motion and strength
Start naproxen 500mg BID
Start acetaminophen; titrate to 1.3g TID as needed for pain control
Start topical capsaicin cream
Refer for PT and start aerobic/strength training program
Patient education
Pt counseled about importance of exercise-based therapy
BMI >25; pt counseled about weight loss to reduce pain
For refractory pain consider
Corticosteroid injections for short-term relief
Tramadol 50 mg q6h
Referral to orthopedics
Icing knees does not improve pain
Knee arthroscopy
Choosing Wisely: Avoid routinely performing arthroscopy with lavage and/or debridement in patients with a primary diagnosis of symptomatic osteoarthritis of the knee
Acute physical therapy is as effective as arthroscopy for improving pain and function
Rule out history of GI ulcers/bleeding and evaluate renal function (BMP) before starting chronic NSAIDs
Pain relief from corticosteroid injections lasts approximately 2 weeks
Lateral wedge insoles, glucosamine/chondroitin supplementation, and hyaluronic acid injections are not recommended for pain control
Femoral Neck Stress Fracture: Female with h/o osteopenia risk factors presents with deep anterolateral hip/groin pain with weight bearing after sudden increase in physical activity. No fevers. Pain with greater trochanter palpation, active leg raise, log roll test, hopping.
X-ray showing cortical disruption
MRI showing early bony edema
Refer to orthopedics; evaluate for management with PT vs. surgery
Pt advised to increase vitamin D intake
Femoroacetabular Impingement: Pt with h/o athletic involvement presents with insidious onset anterolateral hip pain provoked by rising from seated position. Positive FADIR and FABER tests on exam.
Radiography shows Cam or pincer deformity, acetabular retroversion, coxa profunda
PT x2-3 months; refer to orthopedics if no improvement s/p PT
Hip Labral Tear: Pt with h/o hip dislocation presents with painful hip catching/clicking with weight bearing. Pain radiates to lateral hip/anterior thigh/groin/buttock; no fevers. Antalgic gait, loss of internal rotation, positive FADIR and FABER tests on exam.
Consider hip x-ray prior and or MRI prior to magnetic resonance arthrography
Refer to orthopedics pending imaging
Notes
FADIR test
Knee flexion; adduction and internal rotation of leg
Sensitivity: 75-96%
FABER
Knee flexion; abduction and external rotation of leg
Sensitivity: 88%
Magnetic resonance arthrography
Gold standard test
Sensitivity 90%, accuracy 91%
Hip Osteonecrosis: Elderly pt with h/o limited motion presents with gradual onset of constant/deep/aching hip stiffness worse with prolonged standing/weight bearing. Decreased ROM and pain with extremes of motion on exam.
Plain radiographs show asymmetrical joint-space narrowing, osteophytes, subchondral sclerosis/cyst formation
Nonpharmacologic intervention: Weight loss (5% or more), exercise, physical therapy
Acetaminophen 650 to 1,000 mg four times per day
BMP to evaluate renal function prior to starting regular NSAID use
Ibuprofen 600 mg TID PRN, Naproxen 500 mg BID PRN, Diclofenac 50 mg TID PRN
Intra-articular lidocaine/triamcinolone (10mg) injection
Refer to surgery
Iliopsoas Bursitis: Pt with h/o athletic involvement presents with anterior hip pain. Reports intermittent catching/snapping/popping sensation; no fevers. Pain/snapping sensation with hip extension on exam.
No bony involvement on radiography
U/S showing bursitis, tendinopathy with fluid collection
Conservative management x4-6 weeks; pt advised to use NSAIDs, ice, heating pad for pain relief PRN
Deep bursa involvement: Refer to orthopedics as corticosteroid injection may provide additional relief
[3-8 y/o child] vs. [adult with h/o DM, RA, recent hip surgery] presents with acute onset, atraumatic anterior hip pain. Reports fevers; non-weight bearing due to pain. Unilateral limited ROM, positive log roll test.
Obtain CBC, ESR, CRP
Obtain MRI to differentiate septic arthritis vs. transient synovitis
If no evidence of septic arthritis, start ibuprofen
If effusion present on MRI, aspirate and send for culture
If MRI non-diagnostic, consider arthrocentesis of affected joint
Start ibuprofen
Notes
Commonly occurs in two populations
Pediatrics
Common between ages 4-11 years
Most common between ages 3-8 years
Adults with risk factors including
Diabetes mellitus
Rheumatoid arthritis
Recent hip surgery
Diagnosis
Fever only occurs in 60% of patients and is less common in the immunocompromised and elderly
Probability of a septic hip:
Weight bearing and CRP < 20: < 1%
Non-weight bearing and CRP > 20: 74%
Arthrocentesis is the diagnostic test of choice; imaging is not sensitive enough to rule out the condition
Ibuprofen shortens duration of transient synovitis; dosing will be age-dependent
Piriformis syndrome: Pt with no h/o trauma presents with buttock pain with posterior thigh radiation. Pain worse with sitting/walking. No weakness, bowel/bladder dysfunction. Positive log roll test, sciatic notch tenderness on exam.
MRI shows no disc herniation
Refer to physical therapy
Consider orthopedics referral if pain does not improve s/p PT
Sacroiliac joint dysfunction: Pt with h/o minor sacral injury presents with posterior hip pain localized to sacroiliac joint that radiates to lumbar back/buttock/groin. Pt is currently pregnant. Sacroiliac pain elicited with palpation, positive FABER test.
Tylenol PRN for pain
Re-evaluate if pain persists s/p delivery
Middle-aged F with presents with lateral hip pain that radiates down lateral thigh. Trendelenburg gait and pain with palpation over greater trochanter on exam.
Dynamic U/S showing iliotibial band snapping over greater trochanter
Acetaminophen 2g/day x2 weeks followed by NSAIDs if pain persists
Pain persisting for 4+ weeks: Local injection of bursa with 40mg methylprednisolone/5mL 1% lidocaine
Consider surgery if pain persists for greater than 1 year
Obese pt with h/o wearing restrictive clothing presents with numbness/tingling/burning of anterior thigh. Pt advised to lose weight and wear less restrictive clothing
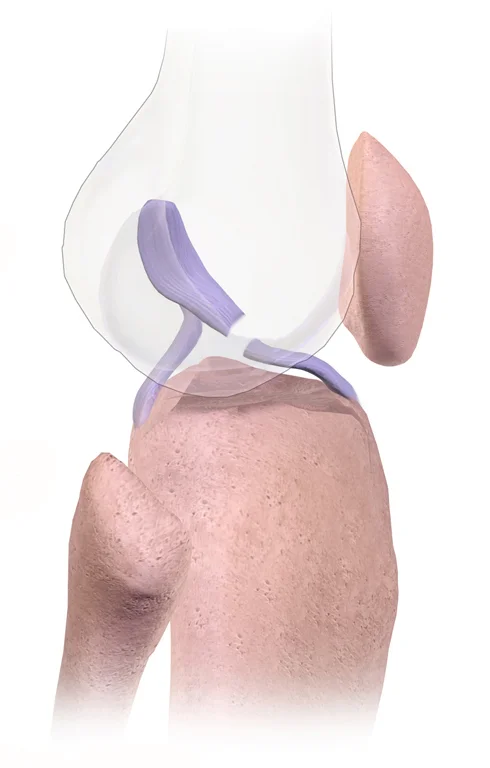
Female athlete involved in running/jumping sports presents with sudden onset knee pain. Reports that she was playing basketball and landed with her foot planted laterally and her upper leg rotated medially when she heard a popping sound. She noted instant knee pain and instability immediately after the injury and was unable to bear weight on the joint. Knee effusion with a ballotable patella and positive Lachman test, anterior drawer test, and lateral pivot-shift test tests on exam.
Suspected ACL injury with knee effusion and/or instability: Obtain MRI
Confirmed ACL tear:
Refer to physical therapy
Pt informed that operative reconstruction is recommended for
Young athletes planning to continue sports involvement
Patients with significant knee instability affecting quality of life
Pt counseled that
Non-operative management may increase risk for chronic pain and future meniscal tears
Risk for degenerative arthritis is the same with operative and non-operative management
Mechanism of injury: Sudden deceleration or change in direction resulting in rotation or valgus knee stress
Injury may produce an audible “pop” and sensation of knee instability
Physical exam
Effusion due to hemarthrosis
Anterior translation with Lachman test and/or anterior drawer test
Lateral pivot-shift test produces posterior movement (reduction) of tibia at 30 to 40 degrees of flexion
Treatment
Patient counseled that arthroscopic meniscal surgery is equivalent to nonoperative management
18 y/o F military recruit with h/o eating disorder, smoking, and consuming > 10 alcoholic drinks per week presents with acute onset tenderness/edema in the lower extremities shortly after starting basic training. Recent physical activity has included running > 25 miles/week. Pain reproducible with ambulation; no tenderness along length of posteromedial tibial shaft.
Imaging
Obtain plain film x-ray; if negative and pain persists, repeat in 2 weeks
Need for immediate diagnosis or suspected 5th metatarsal stress fracture: Obtain MRI
Treatment
Acetaminophen 500 mg QID; consider naproxen 500 mg BID if additional pain control needed
Non-weight bearing crutches for 4 days before transitioning to a walking boot for 4 weeks, and then a rigid sole shoe for an additional 4 weeks
Suspected tibial stress fracture: Recommend pneumatic compression device to reduce time to resumption of full activity
Proximal 5th metatarsal stress (Jones) fracture: Refer to orthopedics
Counseling
Pt counseled that she may resume physical activity upon pain resolution, but that this may require up to 12 weeks
Pt encouraged to adopt balanced diet and engage in cross-training to prevent future stress fractures
Schedule follow-up in 4 weeks
Epidemiology
Risk factors include female sex/female athlete triad, sudden increase in activity (e.g. military recruit), smoking, and > 10 drinks per week
Approximately 75% of stress fractures occur in the tibia/fibula, tarsal navicular bone, or metatarsals
Differential diagnosis
Includes tendinopathy, nerve/artery entrapment syndrome and compartment syndrome
Medial tibial stress syndrome (shin splints) presents with tenderness along posteromedial tibial shaft and no edema
Treatment
NSAIDs may slow healing time
Fifth metatarsal stress fractures may require surgery if located proximally and should be evaluated with MRI
Pt with h/o ankle sprains presents with ankle pain s/p inversion foot injury. Pt is not intoxicated; no h/o peripheral neuropathy. Was able to walk s/p injury. No pain in malleolar zone, at medial/lateral malleolar edge, along posterior fibula. Able to take 4 weight-bearing steps in office without assistance.
Imaging not indicated per Ottawa ankle rules
Start RICE therapy, apply elastic compression bandage
NSAIDs for pain
Pt advised to perform ankle exercises including plantar flexion, dorsiflexion, foot circles
Elderly male patient with history of HTN, cardiovascular disease, and excess meat/pate/beer/high-fructose corn syrup consumption presents with painful first metatarsal joint swelling. Pain present x 1 day and reports similar, previous flares in the same joint. Denies fever, chills, trauma at affected site. Recently started on a diuretic for control of hypertension. Family history positive for gout. Unilateral first metatarsal joint inflammation and tophi noted on exam.
Obtain CBC, uric acid level
Diagnosis
Risk for gout ≥ 82.5% per Acute Gout Diagnosis Rule
Evaluation of joint aspirate with compensated polarized light microscopy shows negatively birefringent monosodium urate crystals
Treatment
Stop thiazide and/or loop diuretic and start losartan
Acute therapy
CrCl > 30: Indomethacin 50 mg TID
CrCl < 30: Colchicine 0.3 mg daily until flare resolves
Concern for pseudogout: Prednisone 40 mg x 4 days, then 20 mg x 4 days, then 10 mg x 4 days
Recurrent gout: Start allopurinol 100 mg qd s/p flare and increase by 100 mg (max 800 mg qd) every 2-4 weeks until serum urate < 6 mg/dL
Counseling
Pt advised to reduce consumption of meats, alcohol, and beverages sweetened with high-fructose corn syrup to reduce risk of gout flares
Pt encouraged to lose weight
Pathophysiology
Due to precipitation of monosodium urate crystals in joint space
Repeat flares can permanently damage joints leading to chronic pain
Risk factors
Age: Present in > 10% of patients > 80 years old
Loop and thiazide diuretics that increase uric acid levels
Purine-rich foods such as red meat, organ meats (liver), and shellfish
Two or more beer or spirit drinks per day; no increase risk with wine
Beverages sweetened with high-fructose corn syrup
Protective factors
Female sex: Hormones increase uric acid excretion (i.e. protective); gout is rare in premenopausal women
Losartan increases uric acid excretion
Diagnosis
Rule out trauma, infection and consider possibility of pseudogout
Diagnosis per American College of Rheumatology requires either
Identification of uric acid crystals in joint aspirate
Presence of ≥ 6 clinical, laboratory, or radiologic findings
Treatment
NSAIDs are first line; consider intra-articular injection to limit systemic absorption
Colchicine has no analgesic properties and has limited effect if started 72 to 96 hours s/p symptom onset
Patients of Korean, Chinese, or Thai descent are at higher risk for a severe skin hypersensitivity reaction when starting allopurinol
Stop thiazide diuretics and start losartan in their place as it lowers gout risk