Vitamin Deficiencies
Vitamin D
Overview
Cholecalciferol synthesized in skin → liver → 25-hydroxyvitamin D → kidney → 1,25-dihydroxycholecalciferol (calcitriol)
Vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol) can both be used for vitamin D supplementation
Calcitriol: Treatment for patients with liver or kidney disease preventing 1,25-dihydroxycholecalciferol synthesis
Screening
Only screen individuals who are at risk for vitamin D deficiency
Recommended screening test: 25-hydroxyvitamin D [25(OH)D]
Documented in patient taking > 60,000 IU/d
Acute symptoms due to hypercalcemia: Confusion, polyuria, polydipsia, anorexia, vomiting, and muscle weakness

Treatment
Cholecalciferol
Pediatric
Breast-fed infants age < 6 months: 400 IU qd
Rickets: Severe vitamin D deficiency in children, rare in developed nations. Treatment regimen includes 50,000 IU vitamin D3 once weekly x 6 weeks followed by maintenance therapy of 400-1000 IU qd to maintain serum vitamin D levels > 30 ng/ml.
Patients with risk factors for vitamin D deficiency: Start 800 IU qd and supplement to 25(OH)D > 30 ng/ml (may require 1500-2000 IU qd)
Primary hyperparathyroidism, malabsorptive syndromes including previous bariatric surgery
Maintenance medications that interfere with vitamin D synthesis (anticonvulsants, antifungals, antiretrovirals)
Patients with multiple sclerosis or at risk of developing multiple sclerosis: 800 IU qd
Geriatric fall and fracture prevention (controversial - see below)
Age > 65 years: 600 IU qd to prevent falls in community dwelling adults
Age > 71 years: 800 IU qd for prevention/treatment of osteoporosis
Calcitriol: Chronic liver or kidney disease
Vitamin D Resources
Based on moderate to high quality of evidence, Cochrane systematic reviews showed that there were some benefits from vitamin D supplementation for pregnant women and asthma patients and no benefits for preventing fractures.
A Review on Vitamin D Deficiency Treatment in Pediatric Patients, J Pediatr Pharmacol Ther.
Folate (Vitamin B9)
Deficiency: Insufficient intake, alcoholism, pregnancy/rapid cellular proliferation, cirrhosis, malabsorption, bariatric surgery, thiamin deficiency
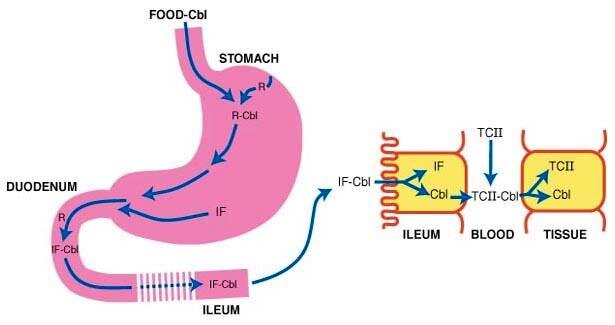
Vitamin B12
Resources: https://www.aafp.org/afp/2003/0301/p979.html#afp20030301p979-b3, https://www.aafp.org/afp/2010/0401/p887.html, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4725715/, https://pubmed.ncbi.nlm.nih.gov/8154512/, https://www.clinicaladvisor.com/home/features/advisor-forum/causes-of-elevated-methylmalonic-acid/
Deficiency etiologies: Insufficient intake, Celiac disease, pernicious anemia, chronic pancreatitis, malabsorption, bariatric surgery)
Pernicious anemia: https://pubmed.ncbi.nlm.nih.gov/26918709/
Intrinsic factor antibodies → impaired B12 absorption → megaloblastic anemia characterized by hypersegmented neutrophils
https://www.youtube.com/watch?v=J8UphjNJljo&ab_channel=HackDentistry
Source: https://emedicine.medscape.com/article/204930-overview