Hepatitis B
Acute Infection
Health care professional with h/o HIV, IV drug use presents with acute onset jaundice. Reports recent needlestick at work and episode of sexual assault. ROS positive for fatigue, poor appetite, N/V, abdominal pain, and dark urine. Denies h/o hepatitis B vaccination. Low-grade fever, jaundice, RUQ tenderness, hepatosplenomegaly on exam.
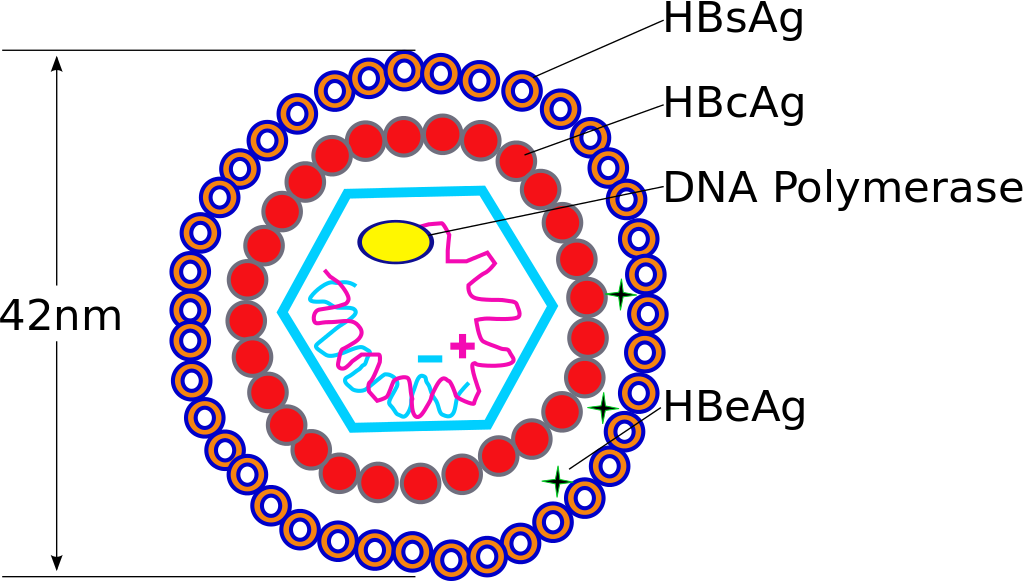
Hepatitis B virus. Source: Transferred by TimVickers from en.wikipedia, Public Domain
Labs
Positive HBsAg, anti-HBc, IgM anti-HBc
Negative anti-HBs
Obtain CBC, CMP, PT/INR
Obtain HBeAg, anti-HBe
Obtain HAV Ab, HCV Ab, hepatitis D Ab, HIV (ELISA Ag/Ab)
Imaging: Obtain RUQ U/S
Treatment: Refer to GI
Healthcare worker with needlestick exposure to HBV positive blood: Administer hepatitis B immunoglobulin and start hepatitis B vaccine series if not vaccinated
Newly diagnosed disease in HBeAg negative pt: Retest HBeAg in 6 months to determine if seroconversion to HbeAg positive state has occurred (see below for treatment of chronic hepatitis B)
Negative HAV Ab: Administer hepatitis A vaccine now and again in 6 months
Administer hepatitis B vaccine to other household members and any sexual contacts
Counseling
Transmission
Pt informed that HBV can be spread via intercourse, exposure to blood of an infected individual, and sharing personal items such as a toothbrush or razor
Pt reassured that HBV is not spread by casual contact (e.g. sharing food, kissing) or breastfeeding
Pt advised to stop drinking alcohol
Pt counseled that monitoring will include regular liver enzyme and HBV DNA level testing

Screening for Chronic Infection
Male pt born in a developing nation with h/o immunosuppression and ESRD requiring dialysis presents for routine health maintenance exam. Reports chronic injection drug use, regular sexual intercourse with men. Previous lab work shows elevated AST, ALT. No documented h/o hepatitis B vaccination. Household contacts include hepatitis B positive individuals. Plan: Obtain HBsAg and anti-HBc.
HBsAg negative, anti-HBc negative: Obtain anti-HBs to determine need for vaccination
HBsAg negative, anti-HBc positive: Obtain anti-HBs to verify immunity status
HBsAg positive, anti-HBc positive: Acute vs. chronic infection
Obtain IgM anti-HBc and anti-HBs to determine acute vs. chronic infection
Refer to sections on evaluation and treatment of acute (above) and chronic (below) hepatitis B infection

Chronic Hepatitis B Evaluation and Treatment
Evaluate for
History of co-infection with HCV, HIV
Personal/family h/o liver disease
History of alcohol use
Signs/symptoms active cirrhosis
Labs
Obtain HbsAg, anti-HBc, IgM anti-HBc, anti-HBs
Obtain HBeAg, anti-HBe, HBV DNA, and HBV genotype
Obtain HAV IgG, HCV Ab, hepatitis D Ab, HIV (ELISA Ag/Ab)
Evaluate liver function: Obtain CBC with diff, CMP, PT/INR
Referrals and Monitoring
Refer to GI for further evaluation
Pt informed that further workup/treatment may include liver biopsy, anti-viral therapy, and/or liver transplant
Counseling: See acute hepatitis B infection (above)
Yearly monitoring for cirrhosis: Obtain alpha-fetoprotein levels and RUQ ultrasound with liver elastography
Refer pt to surveillance program for hepatocellular carcinoma
Treatment
Treatment for patients without cirrhosis
HBeAg positive six months after initial diagnosis
ALT <2x ULN: Continue to monitor
ALT >2x ULN: Start tenofovir 300 mg qd and obtain HBeAg, anti-HBe monthly; continue for 4 months s/p conversion to anti-HBe positive state
HbeAg negative, HBV DNA >2,000 IU, and ALT > 2x ULN: Start tenofovir 300 mg qd and consider continuing treatment indefinitely
Treatment for patients with cirrhosis and HBV DNA >2,000 IU: Start tenofovir 300 mg qd and continue indefinitely
All other patients: Continue to monitor and/or defer to GI recommendations
Notes
Acronyms: HAV, (hepatitis A virus), HBV (hepatitis B virus), HCV (hepatitis C virus), Ag (antigen), Ab (antibody)
Screening
In general, all patients born in Africa and mainland Asia should be screened; see the CDC Yellow Book for all nations with a >2% infection list that qualify for screening
Common risk factors: Dialysis, immunosuppression, increased exposure (e.g. men who have sex with men, IV drug users)
Standard screening tests: HBsAg and anti-HBc
Acute hepatitis B
Liver failure occurs in 1% of patients
Risk for progression chronic disease is greatest in infants (90%) and decreases with age; only 5% of adults progress to chronic disease
Chronic hepatitis B
Considered chronic when infection persists >6 months
Each year, 1 in 400 HBV carriers die due to liver complications
Ultimate goal of treatment is to prevent initiation/progression of cirrhosis
Patients without cirrhosis: Initiation primarily determined by seroconversion to anti-HBe and evidence of liver damage
In cirrhosis patients: Initiation determined by evidence of active disease